

Trends in the incidence and outcome of sepsis using data from a Japanese nationwide medical claims database-the Japan Sepsis Alliance (JaSA) study group
- PMID: 34530884
- PMCID: PMC8444487
- DOI: 10.1186/s13054-021-03762-8
Trends in the incidence and outcome of sepsis using data from a Japanese nationwide medical claims database-the Japan Sepsis Alliance (JaSA) study group
Abstract
Background: Trends in the incidence and outcomes of sepsis using a Japanese nationwide database were investigated.
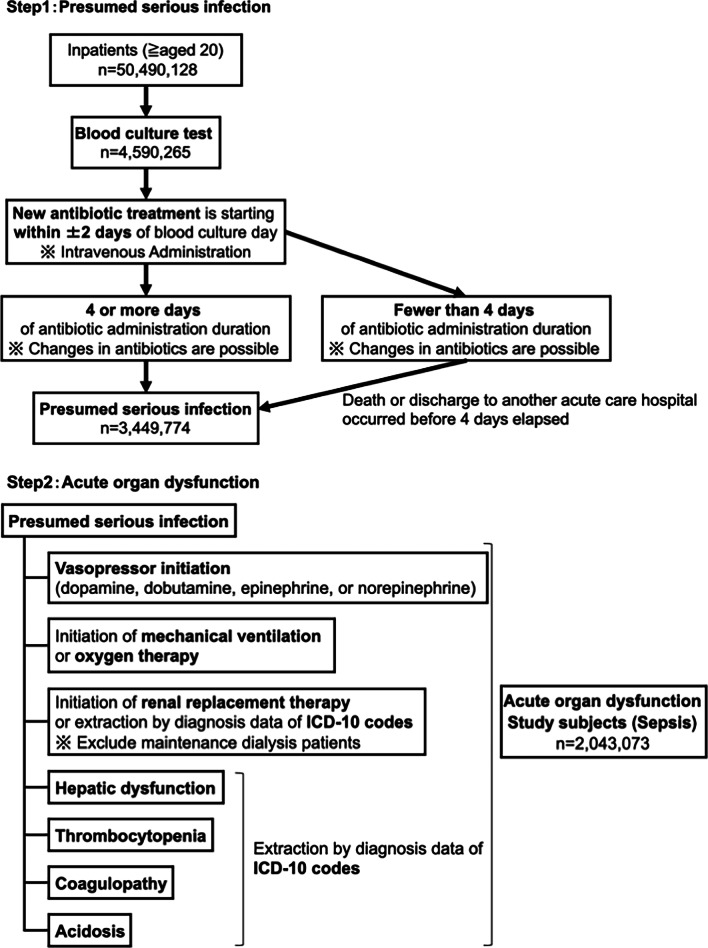
Methods: This was a retrospective cohort study. Adult patients, who had both presumed serious infections and acute organ dysfunction, between 2010 and 2017 were extracted using a combined method of administrative and electronic health record data from the Japanese nationwide medical claim database, which covered 71.5% of all acute care hospitals in 2017. Presumed serious infection was defined using blood culture test records and antibiotic administration. Acute organ dysfunction was defined using records of diagnosis according to the international statistical classification of diseases and related health problems, 10th revision, and records of organ support. The primary outcomes were the annual incidence of sepsis and death in sepsis per 1000 inpatients. The secondary outcomes were in-hospital mortality rate and length of hospital stay in patients with sepsis.
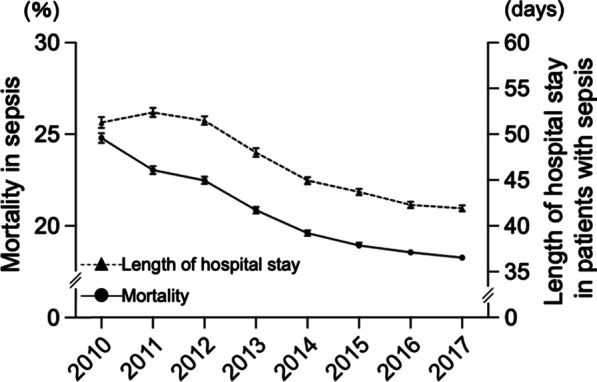
Results: The analyzed dataset included 50,490,128 adult inpatients admitted between 2010 and 2017. Of these, 2,043,073 (4.0%) patients had sepsis. During the 8-year period, the annual proportion of patients with sepsis across inpatients significantly increased (slope = + 0.30%/year, P < 0.0001), accounting for 4.9% of the total inpatients in 2017. The annual death rate of sepsis per 1000 inpatients significantly increased (slope = + 1.8/1000 inpatients year, P = 0.0001), accounting for 7.8 deaths per 1000 inpatients in 2017. The in-hospital mortality rate and median (interquartile range) length of hospital stay significantly decreased (P < 0.001) over the study period and were 18.3% and 27 (15-50) days in 2017, respectively.
Conclusions: The Japanese nationwide data indicate that the annual incidence of sepsis and death in inpatients with sepsis significantly increased; however, the annual mortality rates and length of hospital stay in patients with sepsis significantly decreased. The increasing incidence of sepsis and death in sepsis appear to be a significant and ongoing issue.
Keywords: Blood culture; Epidemiology; ICD-10; Organ dysfunction; Sepsis-3.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Rudd KE, Johnson SC, Agesa KM, Shackelford KA, Tsoi D, Kievlan DR, Colombara DV, Ikuta KS, Kissoon N, Finfer S, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the global burden of disease study. Lancet. 2020;395(10219):200–211. doi: 10.1016/S0140-6736(19)32989-7. - DOI - PMC - PubMed
-
- Abe T, Ogura H, Shiraishi A, Kushimoto S, Saitoh D, Fujishima S, Mayumi T, Shiino Y, Nakada TA, Tarui T, et al. Characteristics, management, and in-hospital mortality among patients with severe sepsis in intensive care units in Japan: the FORECAST study. Crit Care (Lond Engl) 2018;22(1):322. doi: 10.1186/s13054-018-2186-7. - DOI - PMC - PubMed
-
- Fleischmann C, Scherag A, Adhikari NK, Hartog CS, Tsaganos T, Schlattmann P, Angus DC, Reinhart K. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am J Respir Crit Care Med. 2016;193(3):259–272. doi: 10.1164/rccm.201504-0781OC. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
