

Four-factor prothrombin complex concentrate to reduce allogenic blood product transfusion in patients with major trauma, the PROCOAG trial: study protocol for a randomized multicenter double-blind superiority study
- PMID: 34530886
- PMCID: PMC8444177
- DOI: 10.1186/s13063-021-05524-x
Four-factor prothrombin complex concentrate to reduce allogenic blood product transfusion in patients with major trauma, the PROCOAG trial: study protocol for a randomized multicenter double-blind superiority study
Abstract
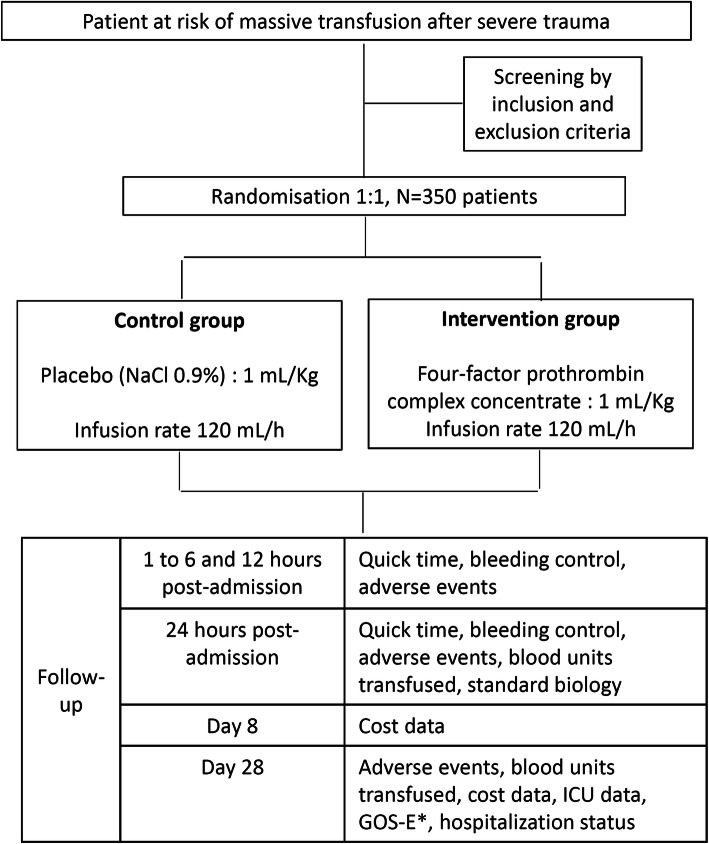
Background: Optimal management of severe trauma patients with active hemorrhage relies on adequate initial resuscitation. Early administration of coagulation factors improves post-traumatic coagulation disorders, and four-factor prothrombin complex concentrate (PCC) might be useful in this context. Our main hypothesis is that four-factor PCC in addition to a massive transfusion protocol decreases blood product consumption at day 1 in severe trauma patients with major bleeding.
Methods: This is a prospective, randomized, multicenter, double-blind, parallel, controlled superiority trial. Eligible patients are trauma patients with major bleeding admitted to a French level-I trauma center. Patients randomized in the treatment arm receive 1 mL/kg (25 IU/ml of Factor IX/Kg) four-factor PCC within 1-h post-admission while patients randomized in the controlled group receive 1 mL/kg of saline solution 0.9% as a placebo. Treatments are given as soon as possible using syringe pumps (120 mL/h). The primary endpoint is the amount of blood products transfused in the first 24 h post-admission (including red blood cells, frozen fresh plasma, and platelets). The secondary endpoints are the amount of each blood product transfused in the first 24 h, time to achieve prothrombin time ratio < 1.5, time to hemostasis, number of thrombo-embolic events at 28 days, mortality at 24 h and 28 days, number of intensive care unit-free days, number of ventilator-free days, number of hospital-free days within the first 28 days, hospitalization status at day 28, Glasgow outcome scale extended for patients with brain lesions on initial cerebral imaging, and cost of each strategy at days 8 and 28. Inclusions have started in December 2017 and are expected to be complete by June 2021.
Discussion: If PCC reduces total blood consumption at day 1 after severe trauma, this therapy, in adjunction to a classic massive transfusion protocol, may be used empirically on admission in patients at risk of massive transfusion to enhance coagulation. Moreover, this treatment may decrease blood product-related complications and may improve clinical outcomes after post-traumatic hemorrhage.
Trial registration: ClinicalTrials.gov NCT03218722 . Registered on July 14, 2017.
Keywords: Acute traumatic coagulopathy; Massive transfusion; Prothrombin complex concentrate; Severe trauma.
© 2021. The Author(s).
Conflict of interest statement
PB, JSD, BR, JD, and JFP received payments from LFB, Les Ullis, France, for lectures and educational content. The other author declares no competing interests.
References
-
- Minei JP, Schmicker RH, Kerby JD, Stiell IG, Schreiber MA, Bulger E, Tisherman S, Hoyt DB, Nichol G, Resuscitation Outcome Consortium Investigators Severe traumatic injury: regional variation in incidence and outcome. Ann Surg. 2010;252(1):149–157. doi: 10.1097/SLA.0b013e3181df0401. - DOI - PMC - PubMed
-
- Tisherman SA, Schmicker RH, Brasel KJ, Bulger EM, Kerby JD, Minei JP, Powell JL, Reiff DA, Rizoli SB, Schreiber MA. Detailed description of all deaths in both the shock and traumatic brain injury hypertonic saline trials of the Resuscitation Outcomes Consortium. Ann Surg. 2015;261(3):586–590. doi: 10.1097/SLA.0000000000000837. - DOI - PMC - PubMed
-
- Holcomb JB, Jenkins D, Rhee P, Johannigman J, Mahoney P, Mehta S, Cox ED, Gehrke MJ, Beilman GJ, Schreiber M, Flaherty SF, Grathwohl KW, Spinella PC, Perkins JG, Beekley AC, McMullin N, Park MS, Gonzalez EA, Wade CE, Dubick MA, Schwab CW, Moore FA, Champion HR, Hoyt DB, Hess JR. Damage control resuscitation: directly addressing the early coagulopathy of trauma. J Trauma. 2007;62(2):307–310. doi: 10.1097/TA.0b013e3180324124. - DOI - PubMed
-
- Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM, del Junco D, Brasel KJ, Bulger EM, Callcut RA, Cohen MJ, Cotton BA, Fabian TC, Inaba K, Kerby JD, Muskat P, O'Keeffe T, Rizoli S, Robinson BR, Scalea TM, Schreiber MA, Stein DM, Weinberg JA, Callum JL, Hess JR, Matijevic N, Miller CN, Pittet JF, Hoyt DB, Pearson GD, Leroux B, van Belle G, PROPPR Study Group Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471–482. doi: 10.1001/jama.2015.12. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
