

Fungal central skull-base osteomyelitis: atypical presentation and management issues
- PMID: 34531233
- PMCID: PMC8449942
- DOI: 10.1136/bcr-2021-243530
Fungal central skull-base osteomyelitis: atypical presentation and management issues
Abstract
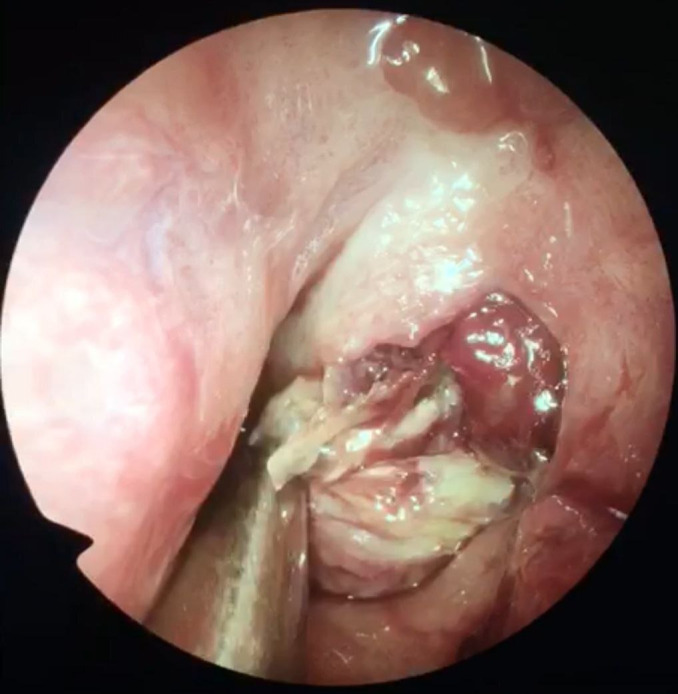
Mucormycosis is a very commonly encountered disease in the sinonasal region in patients with diabetes and immunocompromised status specially in the northern part of the Indian continent. Due to its fulminant nature and involvement in the rhino-orbital-cerebral region, prognosis is poor even after extensive debridement and amphotericin-B therapy. We present a case with diagnosis of sarcoidosis being treated with systemic steroids who developed sudden-onset ptosis and left lateral rectus palsy. On radiological evaluation with MRI, a heterogenously peripherally enhancing lesion was seen in the nasopharynx suggestive of nasopharyngeal abscess. The patient was taken up for emergency surgery; a necrotic lesion with destruction of sphenoid bone, pterygoids and clivus was seen originating in the nasopharynx. The lesion on fungal staining came out to be broad aseptate hyphae suggestive of mucormycosis.
Keywords: drugs: infectious diseases; haematology (drugs and medicines).
© BMJ Publishing Group Limited 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
-
- Baughman RP, Teirstein AS, Judson MA. Clinical characteristics of patients in a case control study of sarcoidosis. Am J Respir Crit Care Med 1885;2001:15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources