

Establishing Surface Correspondence for Post-surgical Cortical Thickness Changes in Temporal Lobe Epilepsy
- PMID: 34531630
- PMCID: PMC8442832
- DOI: 10.1117/12.2580808
Establishing Surface Correspondence for Post-surgical Cortical Thickness Changes in Temporal Lobe Epilepsy
Abstract
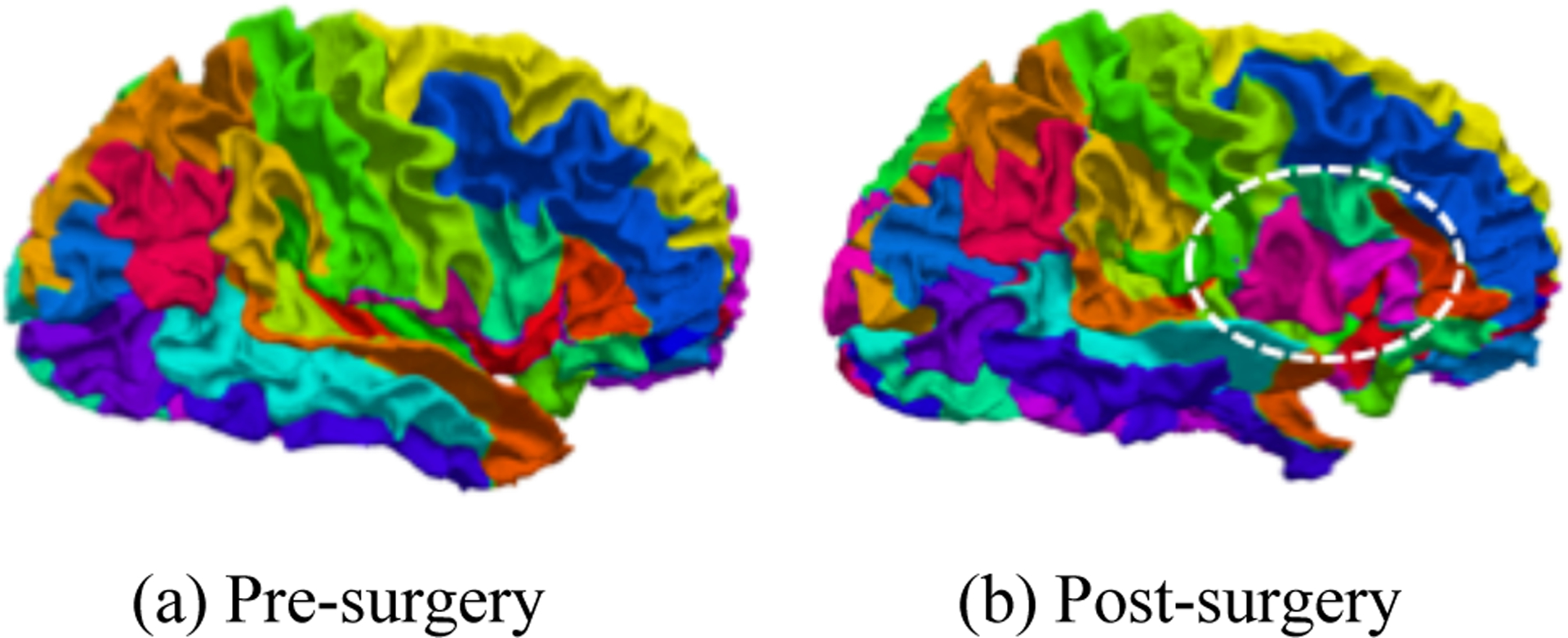
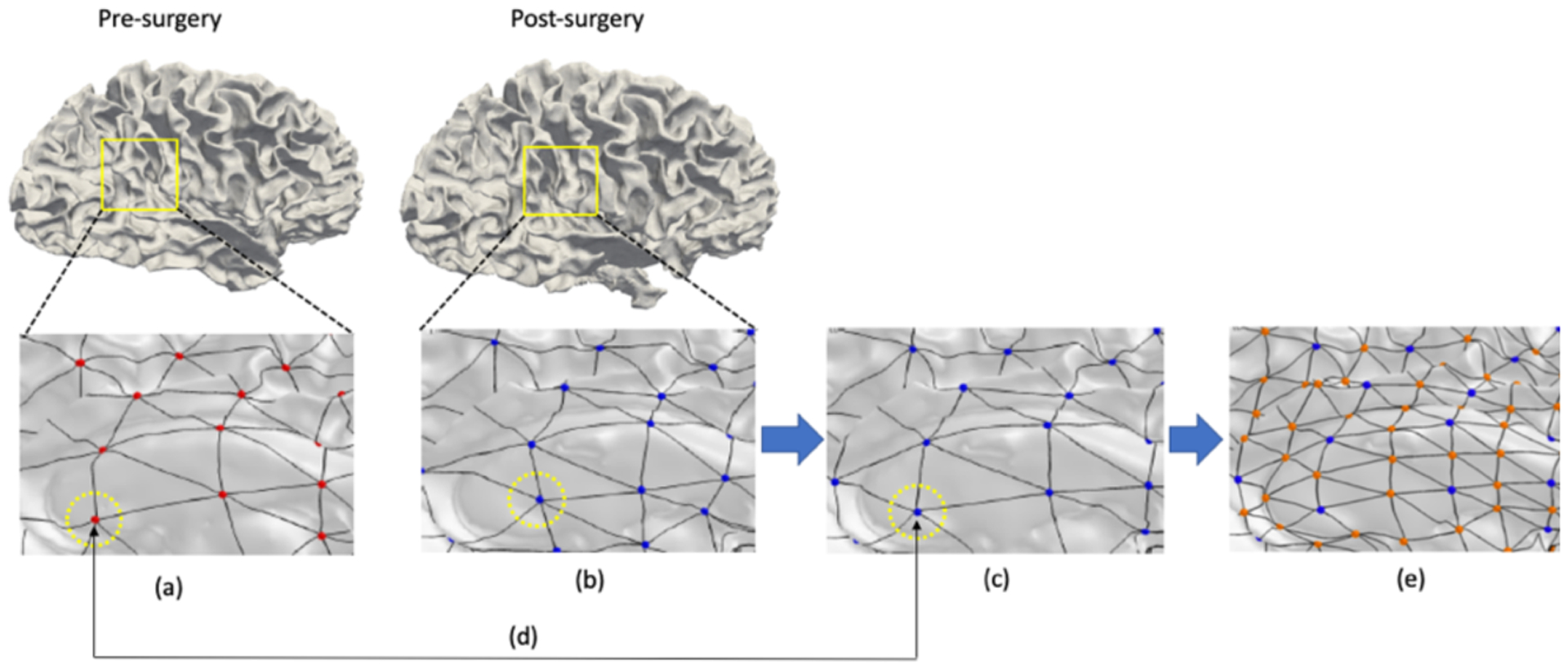
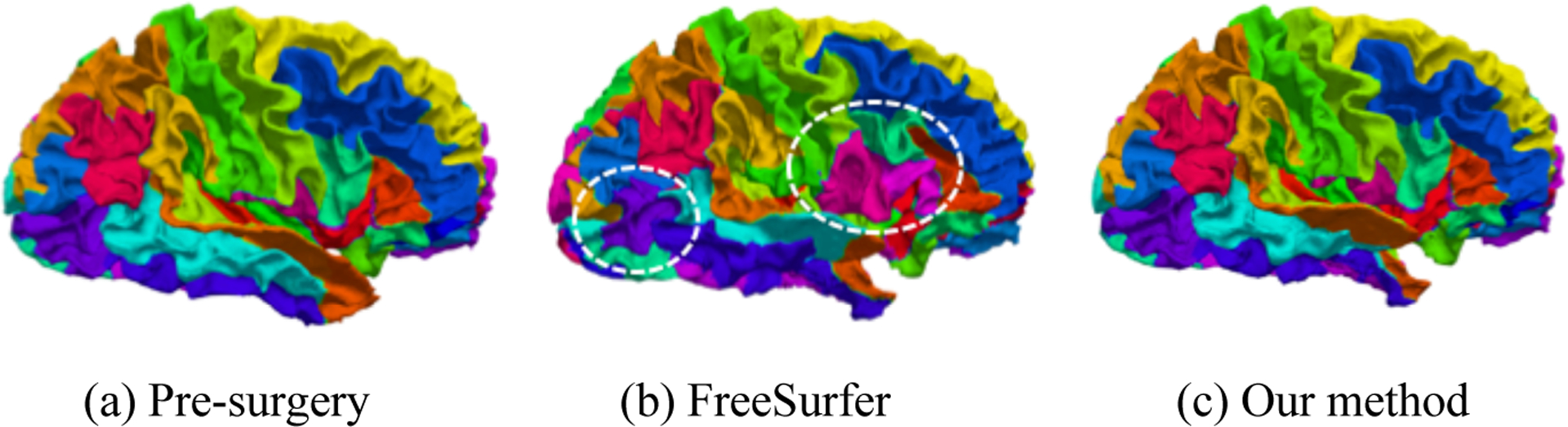
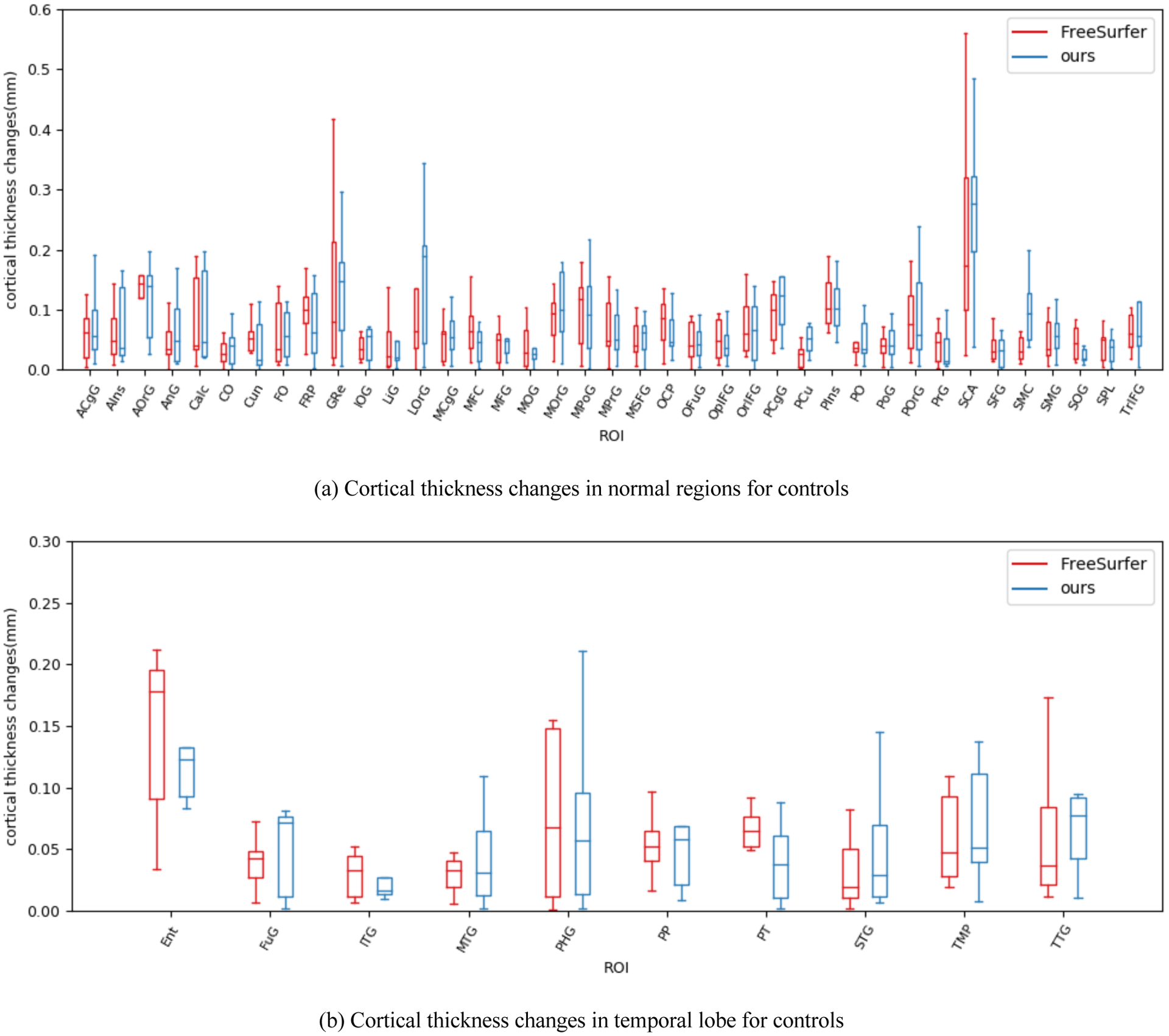
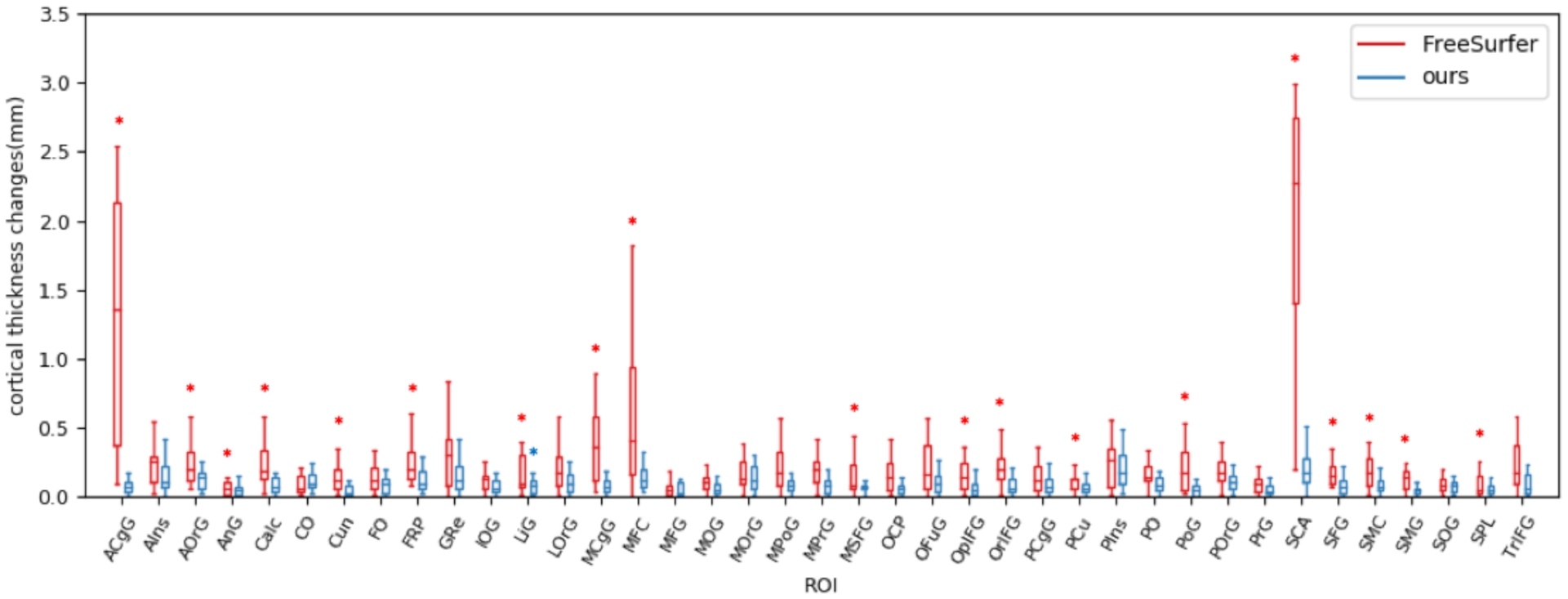
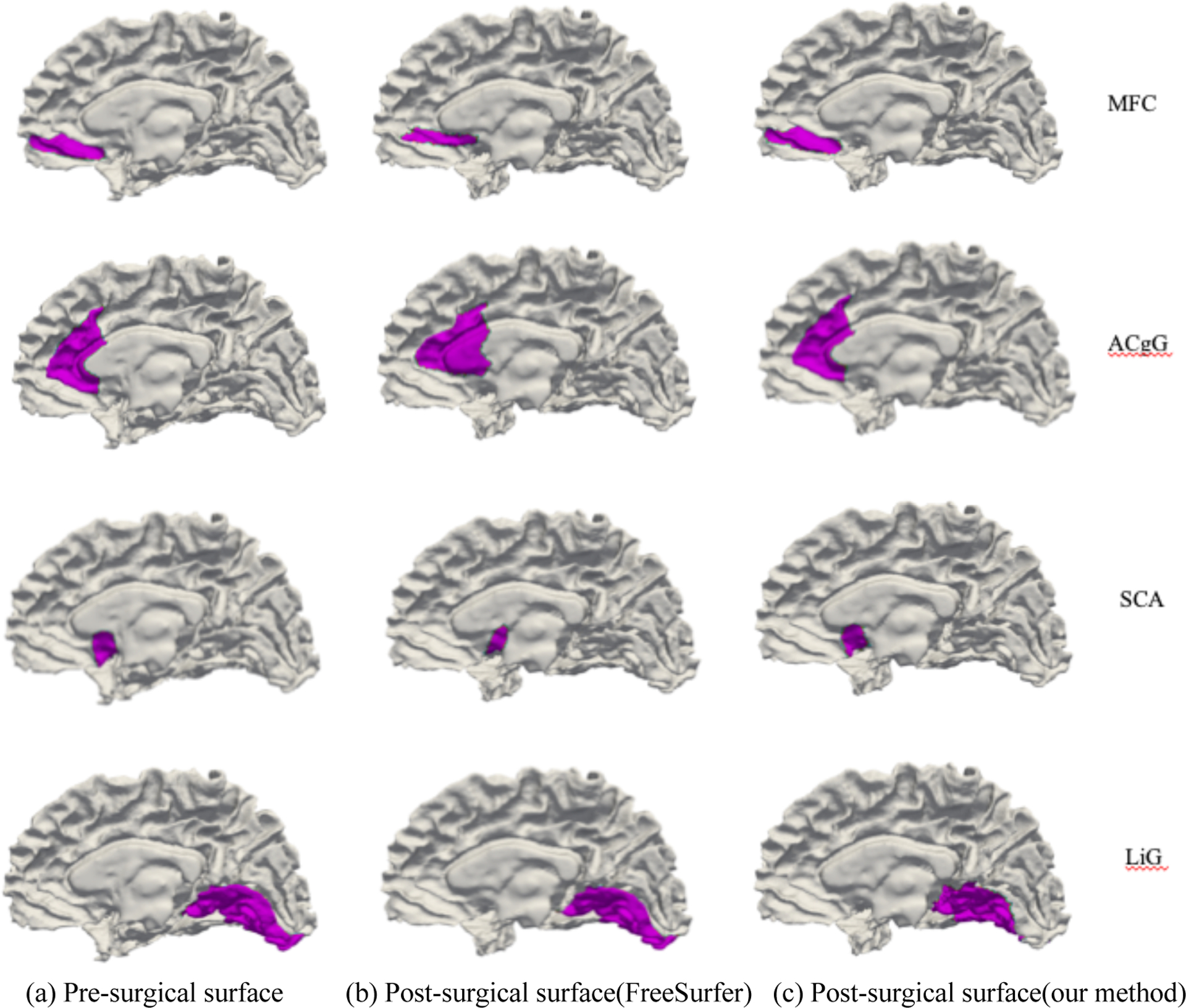
In pre- and post-surgical surface shape analysis, establishing shape correspondence is necessary to investigate the postoperative surface changes. However, structural absence after the operation accompanies focal non-rigid changes, which leads to challenges in existing surface registration methods. In this paper, we present a fully automatic particle-based method to establish surface correspondence that can handle partial structural abnormality in the temporal lobe resection. Our method optimizes the coordinates of points which are modeled as particles on surfaces in a hierarchical way to reduce a chance of being trapped in a local minimum during the optimization. In the experiments, we evaluate the effectiveness of our method in comparison with conventional spherical registration (FreeSurfer) on two scenarios: cortical thickness changes in healthy controls within a short scan-rescan time window and patients with temporal lobe resection. The post-surgical scan is acquired at least 1 year after the presurgical scan. In region of interest-wise (ROI-wise) analysis, no changes on cortical thickness are found in both methods on the healthy control group. In patients, since there is no ground truth available, we instead investigated the disagreement between our method and FreeSurfer. We see poorly matched ROIs and large cortical thickness changes using FreeSurfer. On the contrary, our method shows well-matched ROIs and subtle cortical thickness changes. This suggests that the proposed method can establish a stable shape correspondence, which is not fully captured in a conventional spherical registration.
Keywords: cortical thickness; shape correspondence; surface; temporal lobe epilepsy.
Figures
References
-
- Janszky J, Janszky I, Schulz R, Hoppe M, Behne F, Pannek HW and Ebner A, “Temporal lobe epilepsy with hippocampal sclerosis: predictors for long-term surgical outcome,” Brain 128(2), 395–404 (2005). - PubMed
-
- Wiebe S and Jette N, “Pharmacoresistance and the role of surgery in difficult to treat epilepsy,” Nat. Rev. Neurol 8(12), 669 (2012). - PubMed
-
- Bernhardt BC, Bernasconi N, Concha L and Bernasconi A, “Cortical thickness analysis in temporal lobe epilepsy: reproducibility and relation to outcome,” Neurology 74(22), 1776–1784 (2010). - PubMed
-
- Elliott CA, Gross DW, Wheatley BM, Beaulieu C and Sankar T, “Progressive contralateral hippocampal atrophy following surgery for medically refractory temporal lobe epilepsy,” Epilepsy Res. 125, 62–71 (2016). - PubMed
-
- Fernandes DA, Yasuda CL, Lopes TM, Enrico G, Alessio A, Tedeschi H, de Oliveira E and Cendes F, “Long-term postoperative atrophy of contralateral hippocampus and cognitive function in unilateral refractory MTLE with unilateral hippocampal sclerosis,” Epilepsy Behav. 36, 108–114 (2014). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources