

Newly Diagnosed Atrial Fibrillation in Acute Myocardial Infarction
- PMID: 34533047
- PMCID: PMC8649521
- DOI: 10.1161/JAHA.121.021417
Newly Diagnosed Atrial Fibrillation in Acute Myocardial Infarction
Abstract
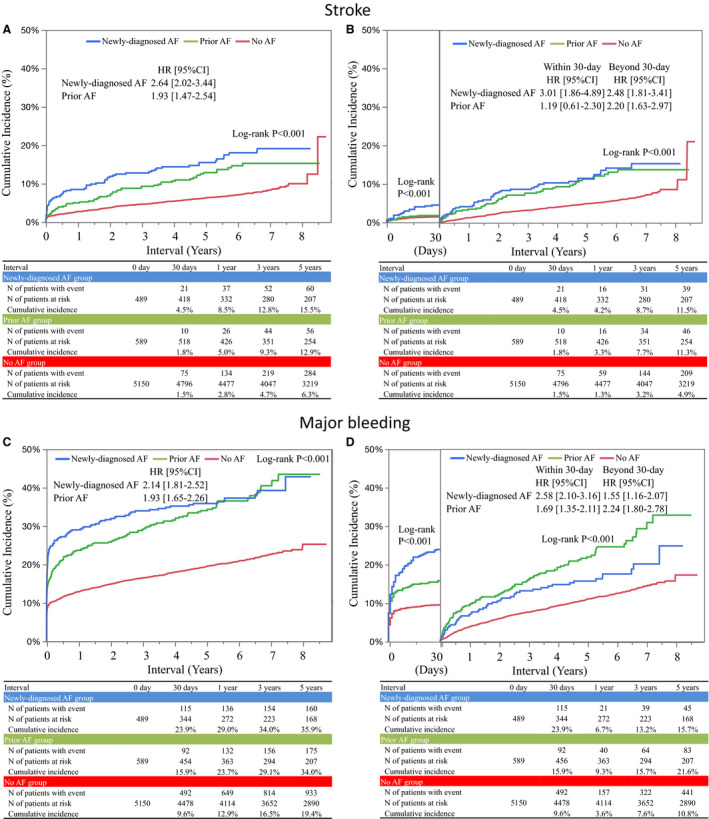
Background It remains controversial whether long-term clinical impact of newly diagnosed atrial fibrillation (AF) in the acute phase of acute myocardial infarction (AMI) is different from that of prior AF diagnosed before the onset of AMI. Methods and Results The current study population from the CREDO-Kyoto AMI (Coronary Revascularization Demonstrating Outcome Study in Kyoto Acute Myocardial Infarction) Registry Wave-2 consisted of 6228 patients with AMI who underwent percutaneous coronary intervention. The baseline characteristics and long-term clinical outcomes were compared according to AF status (newly diagnosed AF: N=489 [7.9%], prior AF: N=589 [9.5%], and no AF: N=5150 [82.7%]). Median follow-up duration was 5.5 years. Patients with newly diagnosed AF and prior AF had similar baseline characteristics with higher risk profile than those with no AF including older age and more comorbidities. The cumulative 5-year incidence of all-cause death was higher in newly diagnosed AF and prior AF than no AF (38.8%, 40.7%, and 18.7%, P<0.001). The adjusted hazard ratios (HRs) for mortality of newly diagnosed AF and prior AF relative to no AF remained significant with similar magnitude (HR, 1.31; 95% CI, 1.12-1.54; P<0.001, and HR, 1.32; 95% CI, 1.14-1.52; P<0.001, respectively). The cumulative 5-year incidence of stroke decreased in the order of newly diagnosed AF, prior AF and no AF (15.5%, 12.9%, and 6.3%, respectively, P<0.001). The higher adjusted HRs of both newly diagnosed AF and prior AF relative to no AF were significant for stroke, with a greater risk of newly diagnosed AF than that of prior AF (HR, 2.05; 95% CI, 1.56-2.69; P<0.001, and HR, 1.33; 95% CI, 1.00-1.78; P=0.048, respectively). The higher stroke risk of newly diagnosed AF compared with prior AF was largely driven by the greater risk within 30 days. The higher adjusted HRs of newly diagnosed AF and prior AF relative to no AF were significant for heart failure hospitalization (HR, 1.73; 95% CI, 1.35-2.22; P<0.001, and HR, 2.23; 95% CI, 1.82-2.74; P<0.001, respectively) and major bleeding (HR, 1.46; 95% CI, 1.23-1.73; P<0.001, and HR, 1.36; 95% CI, 1.15-1.60; P<0.001, respectively). Conclusions Newly diagnosed AF in AMI had risks for mortality, heart failure hospitalization, and major bleeding higher than no AF, and comparable to prior AF. The risk of newly diagnosed AF for stroke might be higher than that of prior AF.
Keywords: acute myocardial infarction; anticoagulation; atrial fibrillation; percutaneous coronary intervention; stroke.
Conflict of interest statement
Dr Shiomi reports personal fees from Boston Scientific, personal fees from Abbot Vascular, and personal fees from Daiichi Sankyo. Dr Morimoto reports modest honoraria from Bayer and Kowa, and modest expert witness from Boston Scientific and Sanofi. Dr Tamura reports personal fees from Daiichi Sankyo and personal fees from Bayer. Dr Furukawa reports personal fees from Daiichi Sankyo, personal fees from Bayer, personal fees from Bristol Myers Squibb, personal fees from Pfizer, and personal fees from Boehringer Ingelheim. Dr Nakagawa reports modest research grant from Abbott Vascular and Boston Scientific, and modest honoraria from Abbott Vascular, Bayer, and Boston Scientific. Dr Kimura reports significant honoraria from Abbott Vascular, and modest honoraria from Astellas, AstraZeneca, Bayer, Boston Scientific, Kowa, and Sanofi. The remaining authors have no disclosures to report.
Figures



References
-
- Vermond RA, Van Gelder IC, Crijns HJ, Rienstra M. Does myocardial infarction beget atrial fibrillation and atrial fibrillation beget myocardial infarction? Circulation. 2015;131:1824–1826. doi: 10.1161/CIRCULATIONAHA.115.016595 - DOI - PubMed
-
- Garg L, Agrawal S, Agarwal M, Shah M, Garg A, Patel B, Agarwal N, Nanda S, Sharma A, Cox D. Influence of atrial fibrillation on outcomes in patients who underwent primary percutaneous coronary intervention for ST‐segment elevation myocardial infarction. Am J Cardiol. 2018;121:684–689. doi: 10.1016/j.amjcard.2017.12.003 - DOI - PubMed
