

The Combination of Beta-Blockers and ACE Inhibitors Across the Spectrum of Cardiovascular Diseases
- PMID: 34533690
- PMCID: PMC10397146
- DOI: 10.1007/s10557-021-07248-1
The Combination of Beta-Blockers and ACE Inhibitors Across the Spectrum of Cardiovascular Diseases
Abstract
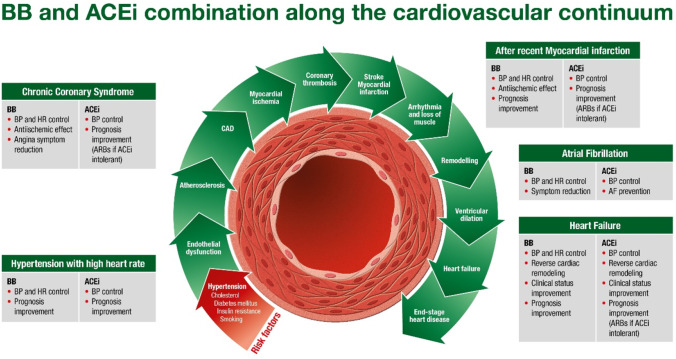
Cardiovascular disease is the leading cause of mortality worldwide, affecting a wide range of patients at different stages across the cardiovascular continuum. Hypertension is one of the earliest risk factors in this continuum and can be controlled in most patients with currently available antihypertensive agents. However, goals are often not met because treatments are not optimized in terms of tailoring therapy to individual patients based on their hypertension subclass and cardiovascular risk profile and initiating early use of adapted-dose, single-pill combinations. In this context, beta-blockers in combination with angiotensin-converting enzyme (ACE) inhibitors are of special interest as a result of their complementary actions on the sympathetic nervous system and renin-angiotensin-aldosterone system, two interlinked pathways that influence cardiovascular risk and disease outcomes. In addition to their antihypertensive actions, beta-blockers are used to manage arrhythmias and treat angina pectoris and heart failure, while ACE inhibitors provide cardioprotection in patients with acute coronary syndromes and treat congestive heart failure. A broad range of patients may therefore receive the combination in routine clinical practice. This paper examines the supporting evidence for beta-blockers and ACE inhibitors in each of the above indications and considers the rationale for combining these agents into a single pill, using data from bisoprolol and perindopril randomized controlled trials as supporting evidence. Combining these established antihypertensive agents into a single pill continues to provide effective blood pressure lowering and improved cardiovascular outcomes while allowing a greater proportion of patients to rapidly achieve treatment targets.
Keywords: Angiotensin II receptor blockers; Angiotensin-converting enzyme inhibitors; Beta-blockers; Coronary artery disease; Hypertension; Renin angiotensin aldosterone system.
© 2021. The Author(s).
Conflict of interest statement
MS received speaking honorarium from Servier. AH declares no competing interest. KN received honoraria from Berlin-Chemie/Menarini, Egis, Idorsia, Gedeon Richter, Krka, Polpharma, Recordati, and Servier.
Figures

References
-
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. GBD-NHLBI-JACC Global burden of cardiovascular diseases writing group. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update From the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi: 10.1016/j.jacc.2020.11.010. - DOI - PMC - PubMed
-
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, et al; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. 2021;143(8):e254-e743 - PubMed
-
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1659–1724. - PMC - PubMed
-
- Williams B, Mancia G, Spiering W, et al. ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018
-
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71(19):2199–2269. doi: 10.1016/j.jacc.2017.11.005. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
