

Upper respiratory tract bacterial-immune interactions during respiratory syncytial virus infection in infancy
- PMID: 34534566
- PMCID: PMC9036861
- DOI: 10.1016/j.jaci.2021.08.022
Upper respiratory tract bacterial-immune interactions during respiratory syncytial virus infection in infancy
Abstract
Background: The risk factors determining short- and long-term morbidity following acute respiratory infection (ARI) due to respiratory syncytial virus (RSV) in infancy remain poorly understood.
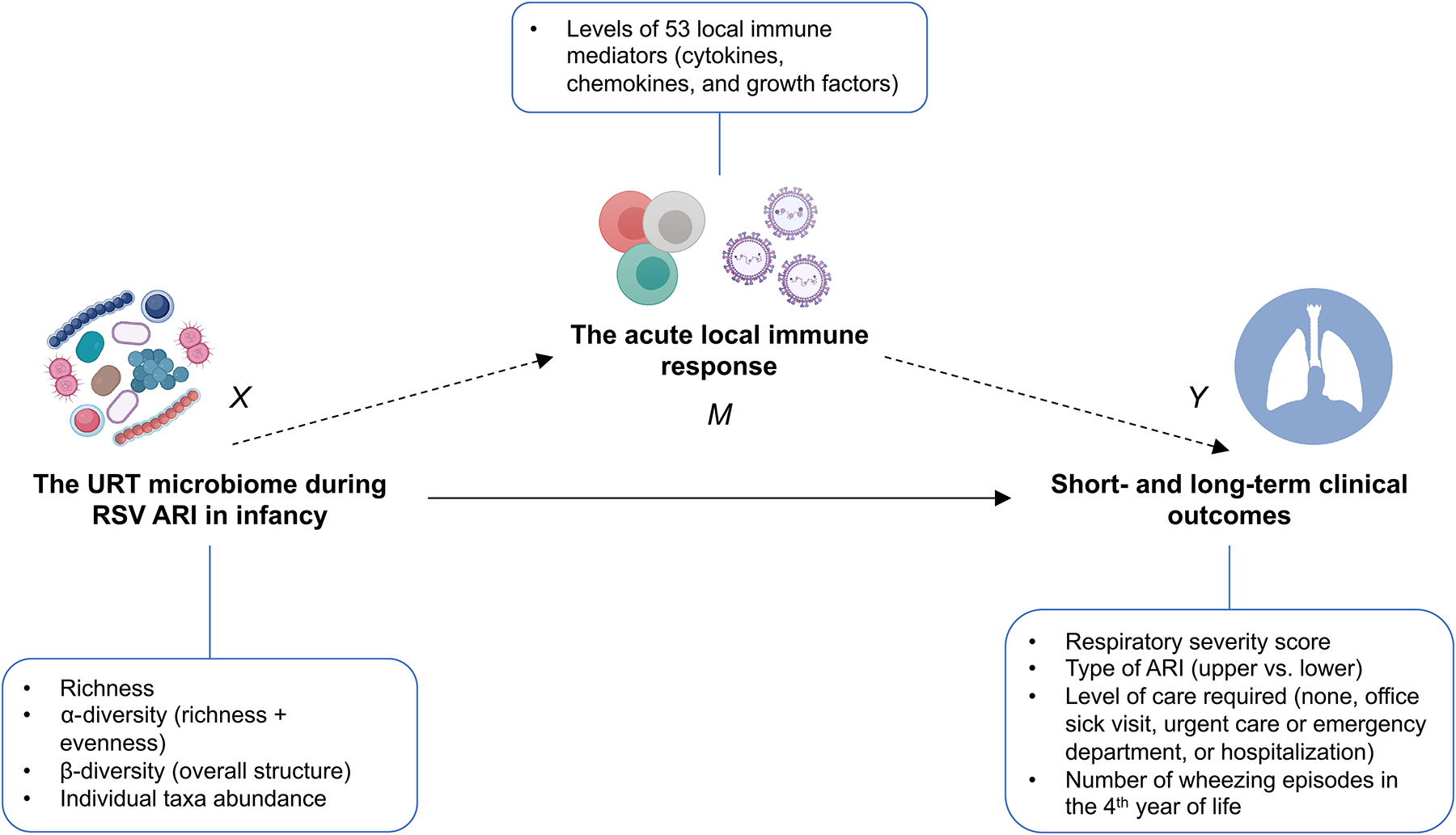
Objectives: Our aim was to examine the associations of the upper respiratory tract (URT) microbiome during RSV ARI in infancy with the acute local immune response and short- and long-term clinical outcomes.
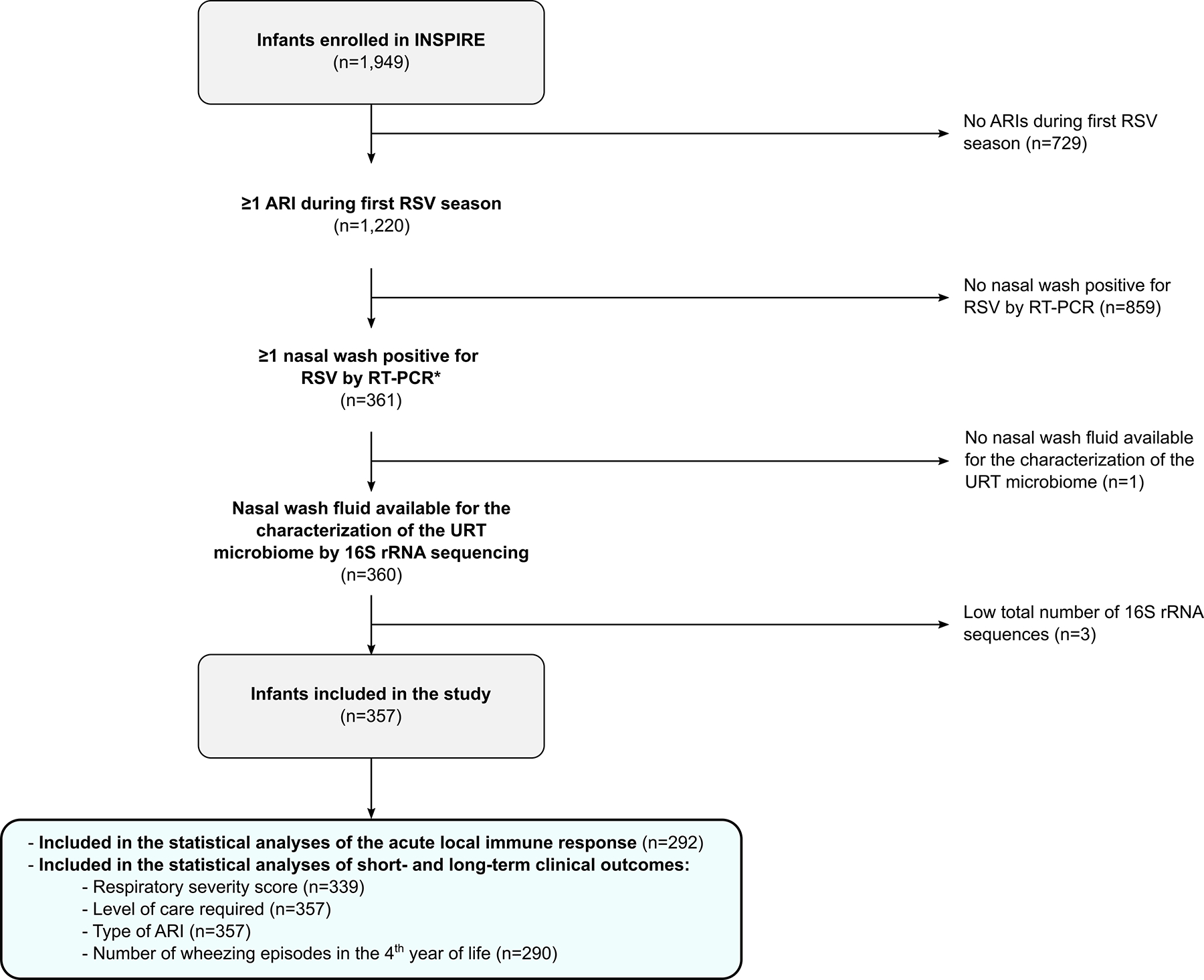
Methods: We characterized the URT microbiome by 16S ribosomal RNA sequencing and assessed the acute local immune response by measuring 53 immune mediators with high-throughput immunoassays in 357 RSV-infected infants. Our short- and long-term clinical outcomes included several markers of disease severity and the number of wheezing episodes in the fourth year of life, respectively.
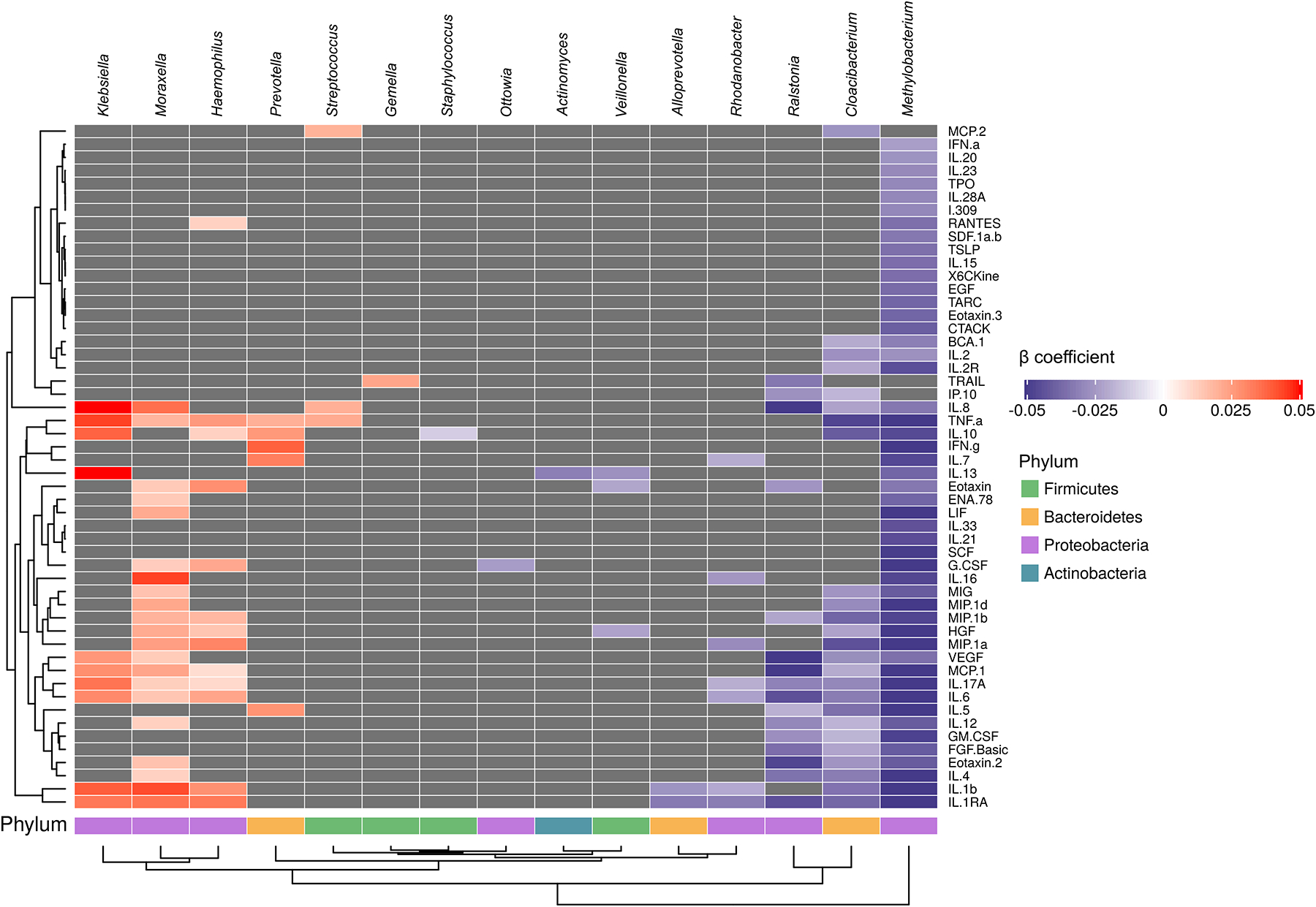
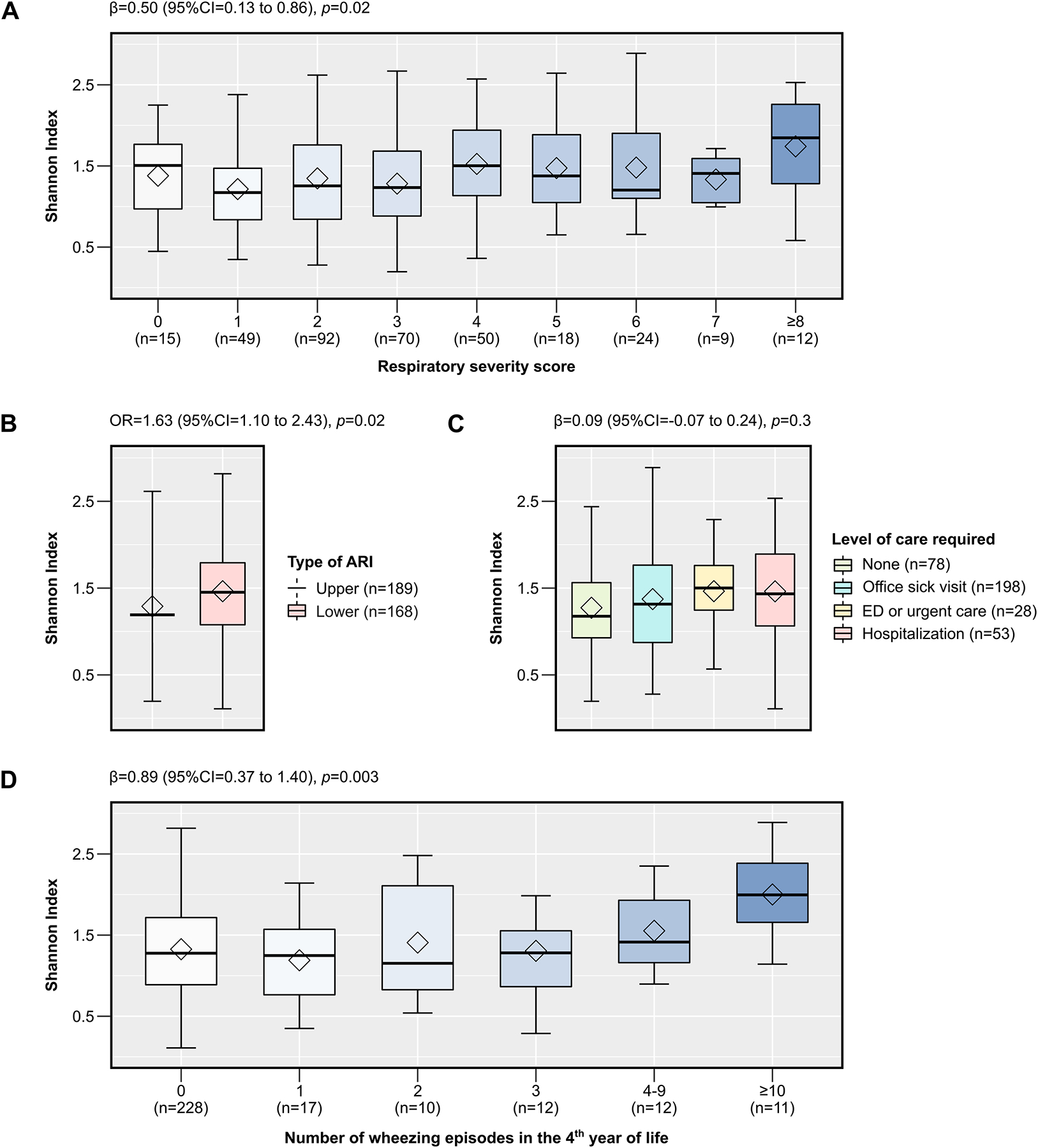
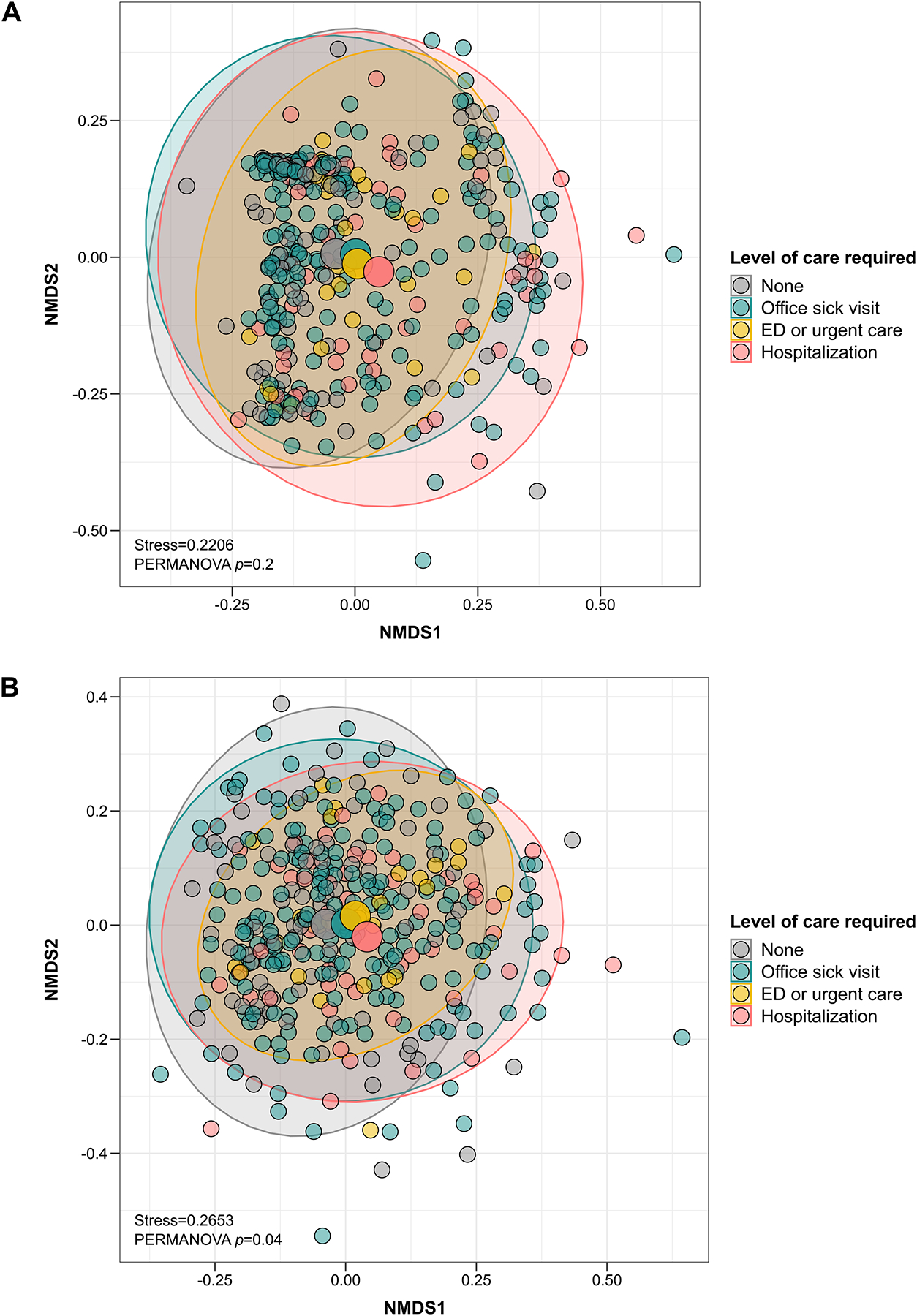
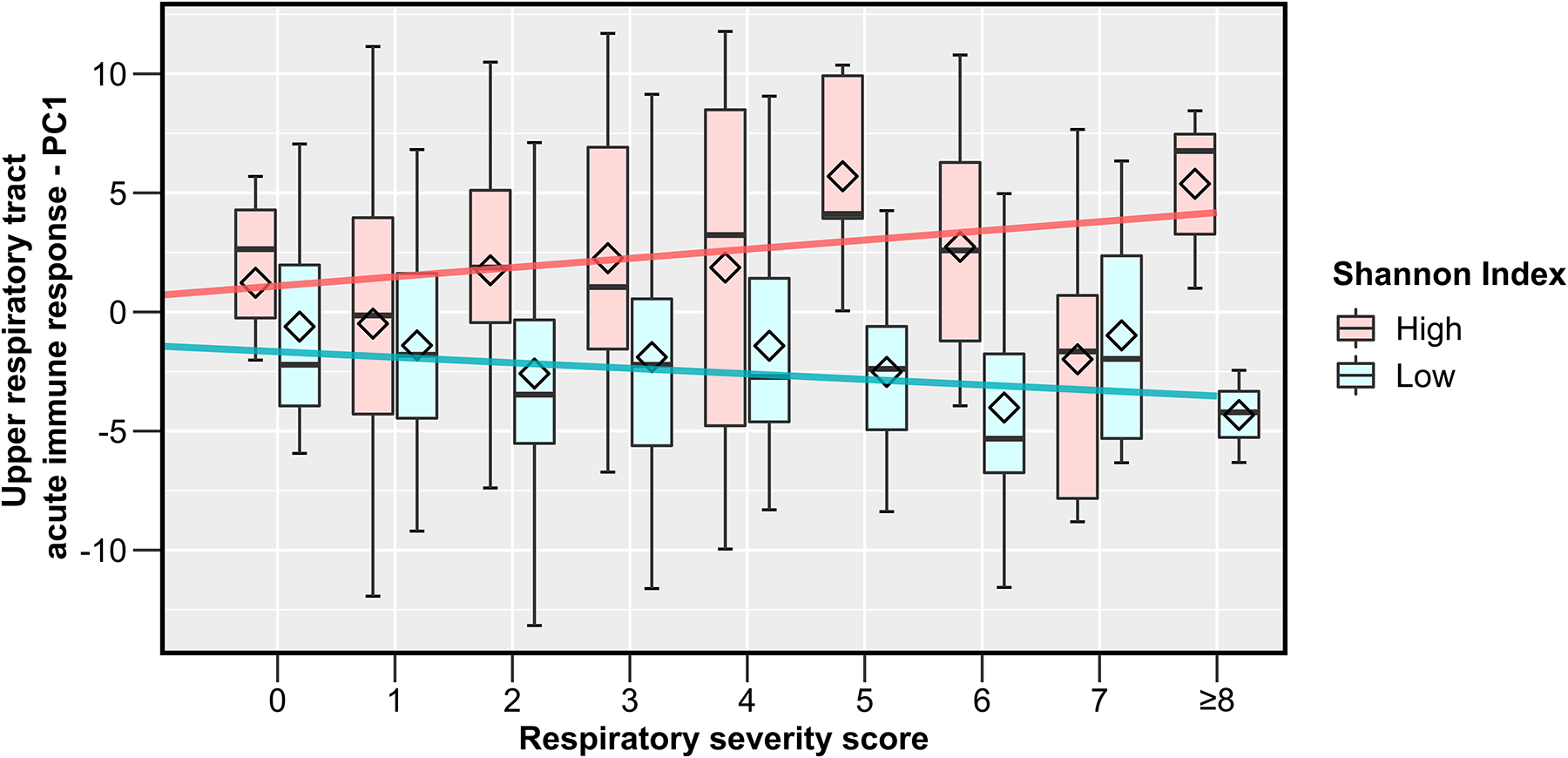
Results: We found several specific URT bacterial-immune mediator associations. In addition, the Shannon ⍺-diversity index of the URT microbiome was associated with a higher respiratory severity score (β =.50 [95% CI = 0.13-0.86]), greater odds of a lower ARI (odds ratio = 1.63 [95% CI = 1.10-2.43]), and higher number of wheezing episodes in the fourth year of life (β = 0.89 [95% CI = 0.37-1.40]). The Jaccard β-diversity index of the URT microbiome differed by level of care required (P = .04). Furthermore, we found an interaction between the Shannon ⍺-diversity index of the URT microbiome and the first principal component of the acute local immune response on the respiratory severity score (P = .048).
Conclusions: The URT microbiome during RSV ARI in infancy is associated with the acute local immune response, disease severity, and number of wheezing episodes in the fourth year of life. Our results also suggest complex URT bacterial-immune interactions that can affect the severity of the RSV ARI.
Keywords: Airway; bronchiolitis; chemokines; cytokines; growth factors; immune response; infancy; mediation; microbiome; nasopharynx; respiratory syncytial virus; severity; wheezing.
Copyright © 2021. Published by Elsevier Inc.
Figures
Comment in
-
Role of nasal microbiota and host response in infants with respiratory syncytial virus infection: Causal questions about respiratory outcomes.J Allergy Clin Immunol. 2022 Mar;149(3):898-900. doi: 10.1016/j.jaci.2021.12.758. Epub 2021 Dec 11. J Allergy Clin Immunol. 2022. PMID: 34906573 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
- UL1 TR000445/TR/NCATS NIH HHS/United States
- K23 HL148638/HL/NHLBI NIH HHS/United States
- R21 AI149262/AI/NIAID NIH HHS/United States
- G20 RR030956/RR/NCRR NIH HHS/United States
- P30 CA068485/CA/NCI NIH HHS/United States
- UL1 RR024975/RR/NCRR NIH HHS/United States
- U19 AI095227/AI/NIAID NIH HHS/United States
- R01 HL146401/HL/NHLBI NIH HHS/United States
- R21 AI142321/AI/NIAID NIH HHS/United States
- K01 HL149989/HL/NHLBI NIH HHS/United States
- R21 AI154016/AI/NIAID NIH HHS/United States
- R01 GM140464/GM/NIGMS NIH HHS/United States
- K24 AI077930/AI/NIAID NIH HHS/United States
- K12 HD087023/HD/NICHD NIH HHS/United States
- P30 EY008126/EY/NEI NIH HHS/United States
- U19 AI110819/AI/NIAID NIH HHS/United States
- HHSN272200900007C/AI/NIAID NIH HHS/United States
- KL2 TR000446/TR/NCATS NIH HHS/United States
- UG3 OD023282/OD/NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
