

The HEART Camp Exercise Intervention Improves Exercise Adherence, Physical Function, and Patient-Reported Outcomes in Adults With Preserved Ejection Fraction Heart Failure
- PMID: 34534664
- PMCID: PMC8920955
- DOI: 10.1016/j.cardfail.2021.09.003
The HEART Camp Exercise Intervention Improves Exercise Adherence, Physical Function, and Patient-Reported Outcomes in Adults With Preserved Ejection Fraction Heart Failure
Abstract
Background: Despite exercise being one of few strategies to improve outcomes for individuals with heart failure with preserved ejection fraction (HFpEF), exercise clinical trials in HFpEF are plagued by poor interventional adherence. Over the last 2 decades, our research team has developed, tested, and refined Heart failure Exercise And Resistance Training (HEART) Camp, a multicomponent behavioral intervention to promote adherence to exercise in HF. We evaluated the effects of this intervention designed to promote adherence to exercise in HF focusing on subgroups of participants with HFpEF and heart failure with reduced ejection fraction (HFrEF).
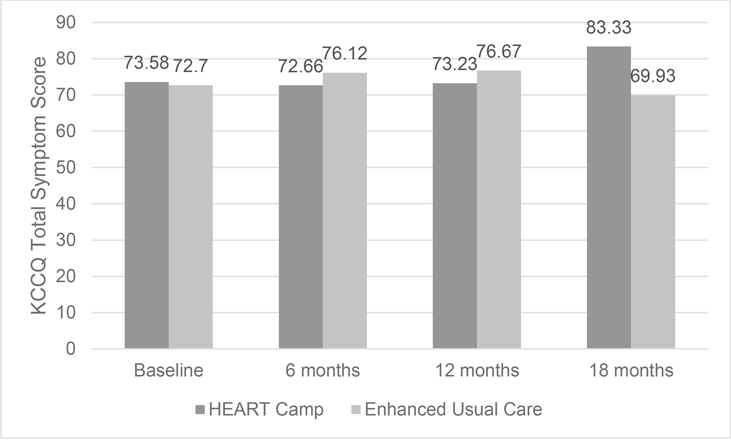
Methods and results: This randomized controlled trial included 204 adults with stable, chronic HF. Of those enrolled, 59 had HFpEF and 145 had HFrEF. We tested adherence to exercise (defined as ≥120 minutes of moderate-intensity [40%-80% of heart rate reserve] exercise per week validated with a heart rate monitor) at 6, 12, and 18 months. We also tested intervention effects on symptoms (Patient-Reported Outcomes Measurement Information System-29 and dyspnea-fatigue index), HF-related health status (Kansas City Cardiomyopathy Questionnaire), and physical function (6-minute walk test). Participants with HFpEF (n = 59) were a mean of 64.6 ± 9.3 years old, 54% male, and 46% non-White with a mean ejection fraction of 55 ± 6%. Participants with HFpEF in the HEART Camp intervention group had significantly greater adherence compared with enhanced usual care at both 12 (43% vs 14%, phi = 0.32, medium effect) and 18 months (56% vs 0%, phi = 0.67, large effect). HEART Camp significantly improved walking distance on the 6-minute walk test (η2 = 0.13, large effect) and the Kansas City Cardiomyopathy Questionnaire overall (η2 = 0.09, medium effect), clinical summary (η2 = 0.16, large effect), and total symptom (η2 = 0.14, large effect) scores. In the HFrEF subgroup, only patient-reported anxiety improved significantly in the intervention group.
Conclusions: A multicomponent, behavioral intervention is associated with improvements in long-term adherence to exercise, physical function, and patient-reported outcomes in adults with HFpEF and anxiety in HFrEF. Our results provide a strong rationale for a large HFpEF clinical trial to validate these findings and examine interventional mechanisms and delivery modes that may further promote adherence and improve clinical outcomes in this population.
Clinical trial registration: URL: https://clinicaltrials.gov/. Unique identifier: NCT01658670.
Keywords: Heart failure; adherence; exercise; heart failure with preserved ejection fraction; heart failure with reduced ejection fraction.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures




References
-
- Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017;70(6):776–803. Accessed Dec 18, 2019. doi: 10.1016/j.jacc.2017.04.025. - DOI - PubMed
-
- Ritchey MD, Maresh S, McNeely J, et al. Tracking cardiac rehabilitation participation and completion among Medicare beneficiaries to inform the efforts of a national initiative. Circ Cardiovasc Qual Outcomes. 2020;13(1):e005902. Accessed Jul 21, 2021. doi: 10.1161/CIRCOUTCOMES.119.005902. - DOI - PMC - PubMed
-
- Maldonado-Martín S, Brubaker PH, Eggebeen J, Stewart KP, Kitzman DW. Association between 6-minute walk test distance and objective variables of functional capacity after exercise training in elderly heart failure patients with preserved ejection fraction: A randomized exercise trial. Arch Phys Med Rehabil. 2017;98(3):600–603. Accessed Apr 25, 2021. doi: 10.1016/j.apmr.2016.08.481. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
