

Association of venous thromboembolism following pediatric traumatic spinal injuries with injury severity and longer hospital stays
- PMID: 34534962
- PMCID: PMC9050628
- DOI: 10.3171/2021.3.SPINE201981
Association of venous thromboembolism following pediatric traumatic spinal injuries with injury severity and longer hospital stays
Abstract
Objective: Venous thromboembolism (VTE) can cause significant morbidity and mortality in hospitalized patients, and may disproportionately occur in patients with limited mobility following spinal trauma. The authors aimed to characterize the epidemiology and clinical predictors of VTE in pediatric patients following traumatic spinal injuries (TSIs).
Methods: The authors conducted a retrospective cohort analysis of children who experienced TSI, including spinal fractures and spinal cord injuries, encoded within the National Trauma Data Bank from 2011 to 2014.
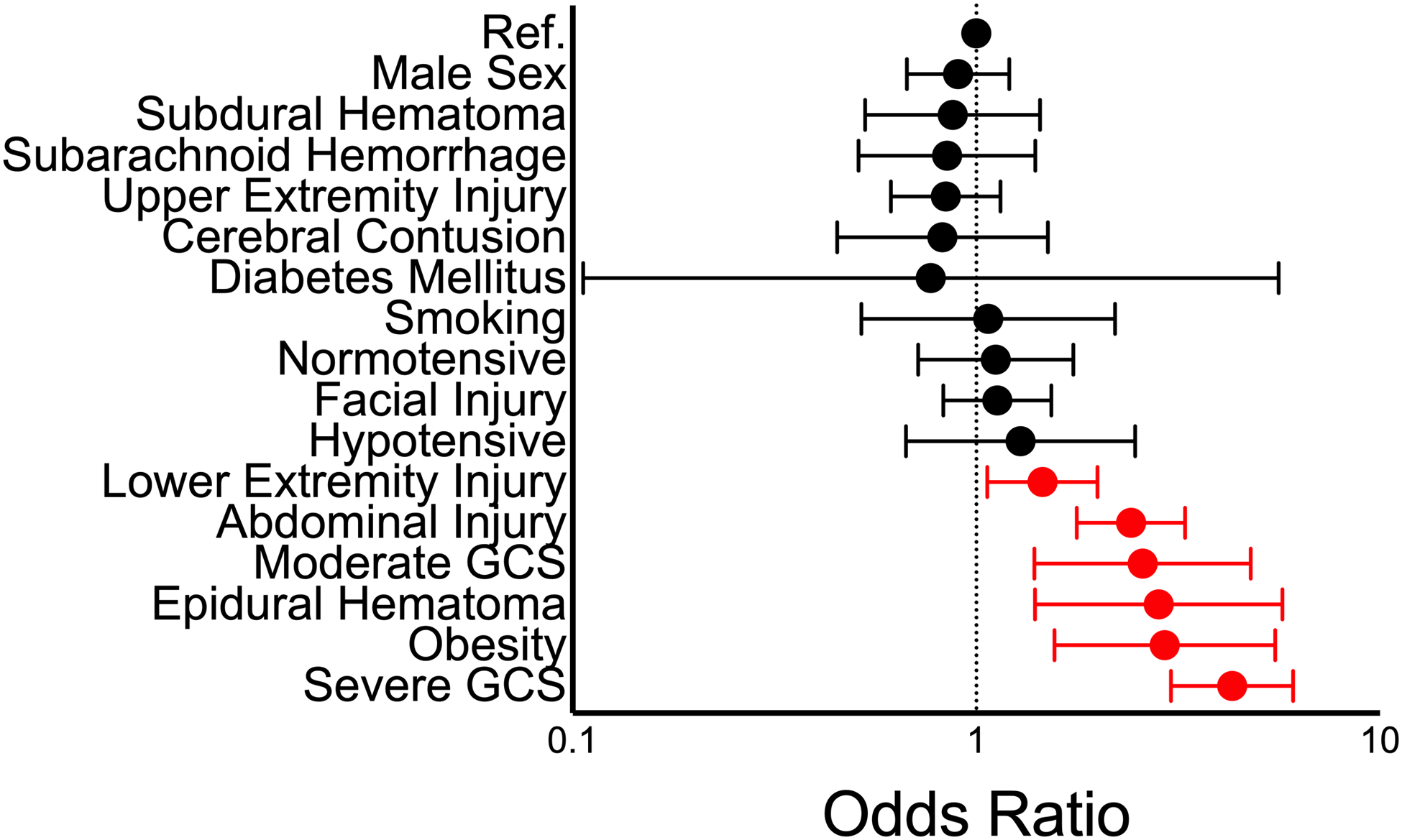
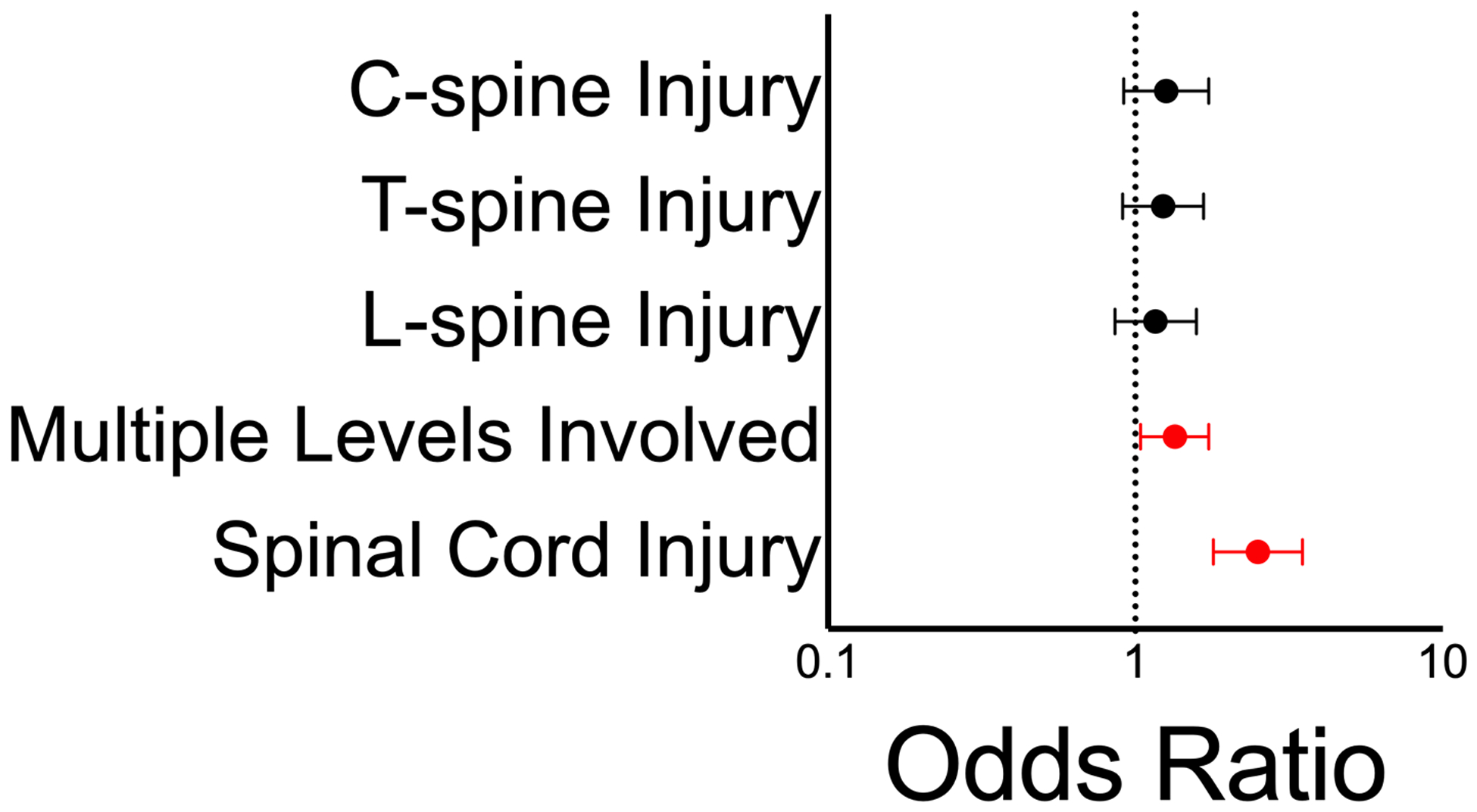
Results: Of the 22,752 pediatric patients with TSI, 192 (0.8%) experienced VTE during initial hospitalization. Proportionally, more patients in the VTE group (77%) than in the non-VTE group (68%) presented following a motor vehicle accident. Patients developing VTE had greater odds of presenting with moderate (adjusted odds ratio [aOR] 2.6, 95% confidence interval [CI] 1.4-4.8) or severe Glasgow Coma Scale scores (aOR 4.3, 95% CI 3.0-6.1), epidural hematoma (aOR 2.8, 95% CI 1.4-5.7), and concomitant abdominal (aOR 2.4, 95% CI 1.8-3.3) and/or lower extremity (aOR 1.5, 95% CI 1.1-2.0) injuries. They also had greater odds of being obese (aOR 2.9, 95% CI 1.6-5.5). Neither cervical, thoracic, nor lumbar spine injuries were significantly associated with VTE. However, involvement of more than one spinal level was predictive of VTE (aOR 1.3, 95% CI 1.0-1.7). Spinal cord injury at any level was also significantly associated with developing VTE (aOR 2.5, 95% CI 1.8-3.5). Patients with VTE stayed in the hospital an adjusted average of 19 days longer than non-VTE patients. They also had greater odds of discharge to a rehabilitative facility or home with rehabilitative services (aOR 2.6, 95% CI 1.8-3.6).
Conclusions: VTE occurs in a low percentage of hospitalized pediatric patients with TSI. Injury severity is broadly associated with increased odds of developing VTE; specific risk factors include concomitant injuries such as cranial epidural hematoma, spinal cord injury, and lower extremity injury. Patients with VTE also require hospital-based and rehabilitative care at greater rates than other patients with TSI.
Keywords: pediatrics; spinal cord injury; trauma; traumatic spinal injury; venous thromboembolism.
Figures


References
-
- Cushman M, Tsai A, Heckbert S, et al. Incidence rates, case fatality, and recurrence rates of deep vein thrombosis and pulmonary embolus: the Longitudinal Investigation of Thromboembolism Etiology (LITE). Thromb Haemost. 2001;86(1)
-
- White RH. The Epidemiology of Venous Thromboembolism. Circulation. 2003;107(23_suppl_1):I-4–I-8. - PubMed
-
- Nielsen H Pathophysiology of venous thromboembolism. 1991:250–253. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
