

Prevention of SARS-CoV-2 (COVID-19) transmission in residential aged care using ultraviolet light (PETRA): a two-arm crossover randomised controlled trial protocol
- PMID: 34535091
- PMCID: PMC8446719
- DOI: 10.1186/s12879-021-06659-7
Prevention of SARS-CoV-2 (COVID-19) transmission in residential aged care using ultraviolet light (PETRA): a two-arm crossover randomised controlled trial protocol
Abstract
Background: SARS-CoV-2 poses a considerable threat to those living in residential aged care facilities (RACF). RACF COVID-19 outbreaks have been characterised by the rapid spread of infection and high rates of severe disease and associated mortality. Despite a growing body of evidence supporting airborne transmission of SARS-CoV-2, current infection control measures in RACF including hand hygiene, social distancing, and sterilisation of surfaces, focus on contact and droplet transmission. Germicidal ultraviolet (GUV) light has been used widely to prevent airborne pathogen transmission. Our aim is to investigate the efficacy of GUV technology in reducing the risk of SARS-CoV-2 infection in RACF.
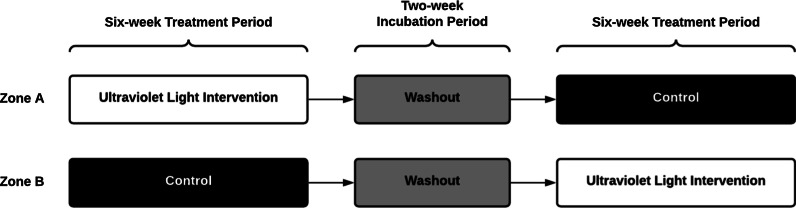
Methods: A multicentre, two-arm double-crossover, randomised controlled trial will be conducted to determine the efficacy of GUV devices to reduce respiratory viral transmission in RACF, as an adjunct to existing infection control measures. The study will be conducted in partnership with three aged care providers in metropolitan and regional South Australia. RACF will be separated into paired within-site zones, then randomised to intervention order (GUV or control). The initial 6-week period will be followed by a 2-week washout before crossover to the second 6-week period. After accounting for estimated within-zone and within-facility correlations of infection, and baseline infection rates (10 per 100 person-days), a sample size of n = 8 zones (n = 40 residents/zone) will provide 89% power to detect a 50% reduction in symptomatic infection rate. The primary outcome will be the incidence rate ratio of combined symptomatic respiratory infections for intervention versus control. Secondary outcomes include incidence rates of hospitalisation for complications associated with respiratory infection; respiratory virus detection in facility air and fomite samples; rates of laboratory confirmed respiratory illnesses and genomic characteristics.
Discussion: Measures that can be deployed rapidly into RACF, that avoid the requirement for changes in resident and staff behaviour, and that are effective in reducing the risk of airborne SARS-CoV-2 transmission, would provide considerable benefit in safeguarding a highly vulnerable population. In addition, such measures might substantially reduce rates of other respiratory viruses, which contribute considerably to resident morbidity and mortality. Trial registration Australian and New Zealand Clinical Trials Registry ACTRN12621000567820 (registered on 14th May, 2021).
Keywords: COVID-19; Germicidal ultraviolet light; Health care quality; Residential aged care; Respiratory virus infection; SARS-CoV-2; Transmission.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
