

A hypolipoprotein sepsis phenotype indicates reduced lipoprotein antioxidant capacity, increased endothelial dysfunction and organ failure, and worse clinical outcomes
- PMID: 34535154
- PMCID: PMC8447561
- DOI: 10.1186/s13054-021-03757-5
A hypolipoprotein sepsis phenotype indicates reduced lipoprotein antioxidant capacity, increased endothelial dysfunction and organ failure, and worse clinical outcomes
Abstract
Objective: Approximately one-third of sepsis patients experience poor outcomes including chronic critical illness (CCI, intensive care unit (ICU) stay > 14 days) or early death (in-hospital death within 14 days). We sought to characterize lipoprotein predictive ability for poor outcomes and contribution to sepsis heterogeneity.
Design: Prospective cohort study with independent replication cohort.
Setting: Emergency department and surgical ICU at two hospitals.
Patients: Sepsis patients presenting within 24 h.
Methods: Measures included cholesterol levels (total cholesterol, high density lipoprotein cholesterol [HDL-C], low density lipoprotein cholesterol [LDL-C]), triglycerides, paraoxonase-1 (PON-1), and apolipoprotein A-I (Apo A-I) in the first 24 h. Inflammatory and endothelial markers, and sequential organ failure assessment (SOFA) scores were also measured. LASSO selection assessed predictive ability for outcomes. Unsupervised clustering was used to investigate the contribution of lipid variation to sepsis heterogeneity.
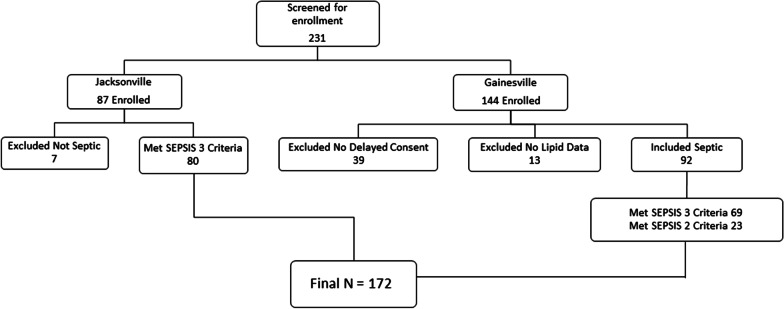
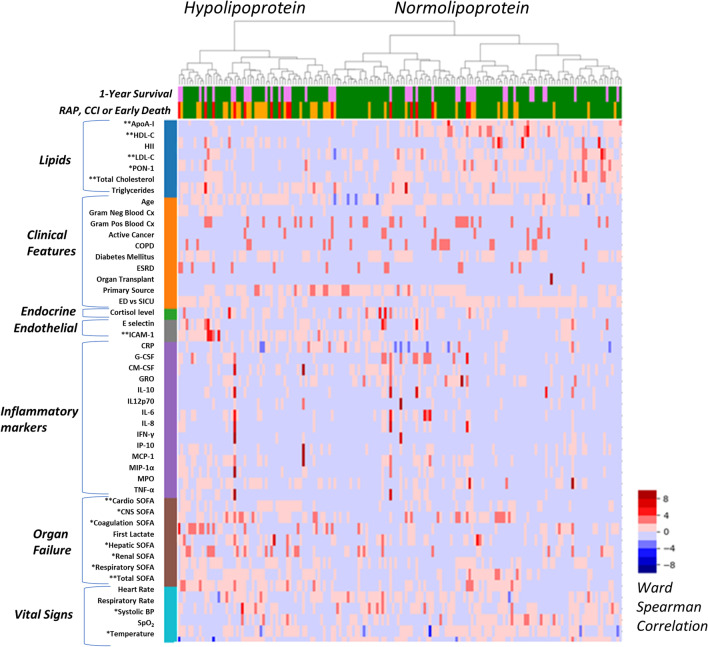
Measurements and main results: 172 patients were enrolled. Most (~ 67%, 114/172) rapidly recovered, while ~ 23% (41/172) developed CCI, and ~ 10% (17/172) had early death. ApoA-I, LDL-C, mechanical ventilation, vasopressor use, and Charlson Comorbidity Score were significant predictors of CCI/early death in LASSO models. Unsupervised clustering yielded two discernible phenotypes. The Hypolipoprotein phenotype was characterized by lower lipoprotein levels, increased endothelial dysfunction (ICAM-1), higher SOFA scores, and worse clinical outcomes (45% rapid recovery, 40% CCI, 16% early death; 28-day mortality, 21%). The Normolipoprotein cluster patients had higher cholesterol levels, less endothelial dysfunction, lower SOFA scores and better outcomes (79% rapid recovery, 15% CCI, 6% early death; 28-day mortality, 15%). Phenotypes were validated in an independent replication cohort (N = 86) with greater sepsis severity, which similarly demonstrated lower HDL-C, ApoA-I, and higher ICAM-1 in the Hypolipoprotein cluster and worse outcomes (46% rapid recovery, 23% CCI, 31% early death; 28-day mortality, 42%). Normolipoprotein patients in the replication cohort had better outcomes (55% rapid recovery, 32% CCI, 13% early death; 28-day mortality, 28%) Top features for cluster discrimination were HDL-C, ApoA-I, total SOFA score, total cholesterol level, and ICAM-1.
Conclusions: Lipoproteins predicted poor sepsis outcomes. A Hypolipoprotein sepsis phenotype was identified and characterized by lower lipoprotein levels, increased endothelial dysfunction (ICAM-1) and organ failure, and worse clinical outcomes.
Keywords: Inflammation; Lipids; Lipoprotein; Quality of life; Sepsis; Shock.
© 2021. The Author(s).
Conflict of interest statement
The authors have no competing interests to report. All authors have read Biomed Central’s section on competing interests and have no competing interests to disclose.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- R01GM133815/GM/NIGMS NIH HHS/United States
- P50 GM111152/GM/NIGMS NIH HHS/United States
- KL2TR001429/TR/NCATS NIH HHS/United States
- L30 TR003473/TR/NCATS NIH HHS/United States
- KL2 TR001429/TR/NCATS NIH HHS/United States
- K23GM115690/GM/NIGMS NIH HHS/United States
- P01AI042288/National Institute of Allergy and Infectious Diseases
- K23 GM144802/GM/NIGMS NIH HHS/United States
- P01 AI042288/AI/NIAID NIH HHS/United States
- P50GM111152/GM/NIGMS NIH HHS/United States
- R01 GM133815/GM/NIGMS NIH HHS/United States
- K23 GM115690/GM/NIGMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
