

The United Kingdom Research study into Ethnicity And COVID-19 outcomes in Healthcare workers (UK-REACH): protocol for a prospective longitudinal cohort study of healthcare and ancillary workers in UK healthcare settings
- PMID: 34535484
- PMCID: PMC8450967
- DOI: 10.1136/bmjopen-2021-050647
The United Kingdom Research study into Ethnicity And COVID-19 outcomes in Healthcare workers (UK-REACH): protocol for a prospective longitudinal cohort study of healthcare and ancillary workers in UK healthcare settings
Abstract
Introduction: The COVID-19 pandemic has resulted in significant morbidity and mortality and devastated economies globally. Among groups at increased risk are healthcare workers (HCWs) and ethnic minority groups. Emerging evidence suggests that HCWs from ethnic minority groups are at increased risk of adverse COVID-19-related outcomes. To date, there has been no large-scale analysis of these risks in UK HCWs or ancillary workers in healthcare settings, stratified by ethnicity or occupation, and adjusted for confounders. This paper reports the protocol for a prospective longitudinal questionnaire study of UK HCWs, as part of the UK-REACH programme (The United Kingdom Research study into Ethnicity And COVID-19 outcomes in Healthcare workers).
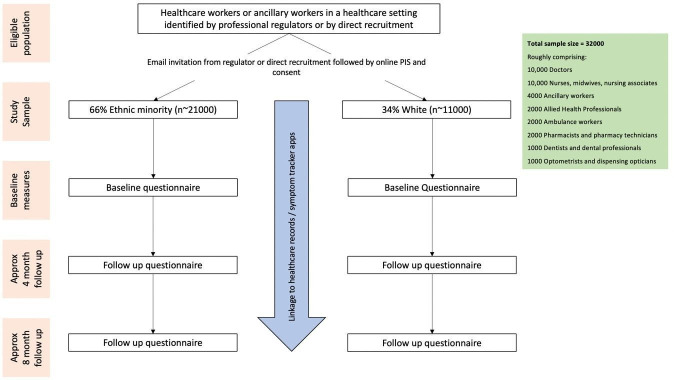
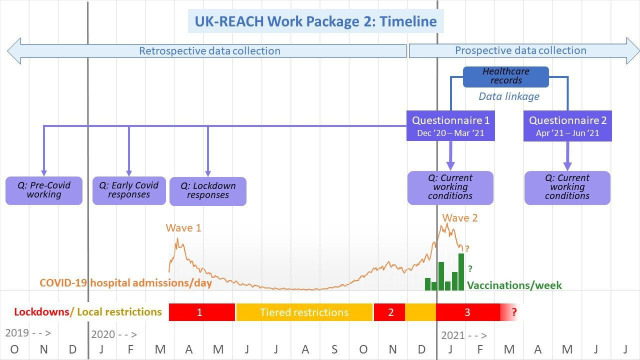
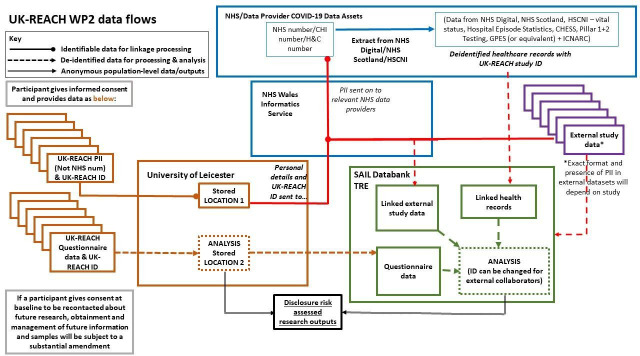
Methods and analysis: A baseline questionnaire will be administered to a national cohort of UK HCWs and ancillary workers in healthcare settings, and those registered with UK healthcare regulators, with follow-up questionnaires administered at 4 and 8 months. With consent, questionnaire data will be linked to health records with 25-year follow-up. Univariate associations between ethnicity and clinical COVID-19 outcomes, physical and mental health, and key confounders/explanatory variables will be tested. Multivariable analyses will test for associations between ethnicity and key outcomes adjusted for the confounder/explanatory variables. We will model changes over time by ethnic group, facilitating understanding of absolute and relative risks in different ethnic groups, and generalisability of findings.
Ethics and dissemination: The study is approved by Health Research Authority (reference 20/HRA/4718), and carries minimal risk. We aim to manage the small risk of participant distress about questions on sensitive topics by clearly participant information that the questionnaire covers sensitive topics and there is no obligation to answer these or any other questions, and by providing support organisation links. Results will be disseminated with reports to Government and papers submitted to pre-print servers and peer reviewed journals.
Trial registration number: ISRCTN11811602; Pre-results.
Keywords: COVID-19; mental health; public health.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: SC is Deputy Medical Director of the General Medical Council, UK Honorary Professor, University of Leicester. KK is Director of the University of Leicester Centre for Black Minority Ethnic Health, Trustee of the South Asian Health Foundation, Chair of the Ethnicity Subgroup of SAGE and Member of Independent SAGE. LVW receives grant funding from GSK and Orion, outside of the submitted work. KRA has served as a paid consultant, providing unrelated methodological and strategic advice, to the pharmaceutical and life sciences industry generally and has received unrelated research funding from Association of the British Pharmaceutical Industry, European Federation of Pharmaceutical Industries & Associations, Pfizer, Sanofi and Swiss Precision Diagnostics. He is a Partner and Director of Visible Analytics Limited, a healthcare consultancy company.
Figures
References
-
- Office for National Statistics . Coronavirus (COVID-19) related deaths by occupation, England and Wales: deaths registered between 9 March and 28 December 2020, 2021. Available: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/...
-
- Ayoubkhani D, Khunti K, Nafilyan V, et al. Epidemiology of post-COVID syndrome following hospitalisation with coronavirus: a retrospective cohort study. medRxiv 2021:2021.01.15.21249885.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical