

The role of hybrid FDG-PET/MRI on decision-making in presurgical evaluation of drug-resistant epilepsy
- PMID: 34537017
- PMCID: PMC8449490
- DOI: 10.1186/s12883-021-02352-z
The role of hybrid FDG-PET/MRI on decision-making in presurgical evaluation of drug-resistant epilepsy
Abstract
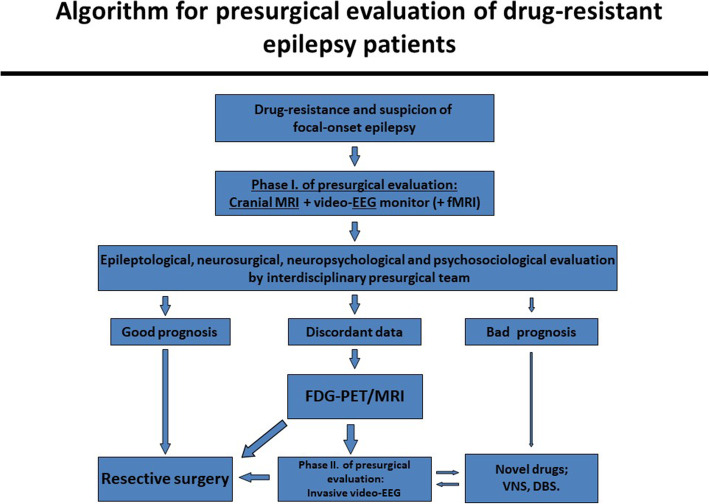
Background: When MRI fails to detect a potentially epileptogenic lesion, the chance of a favorable outcome after epilepsy surgery becomes significantly lower (from 60 to 90% to 20-65%). Hybrid FDG-PET/MRI may provide additional information for identifying the epileptogenic zone. We aimed to investigate the possible effect of the introduction of hybrid FDG-PET/MRI into the algorithm of the decision-making in both lesional and non-lesional drug-resistant epileptic patients.
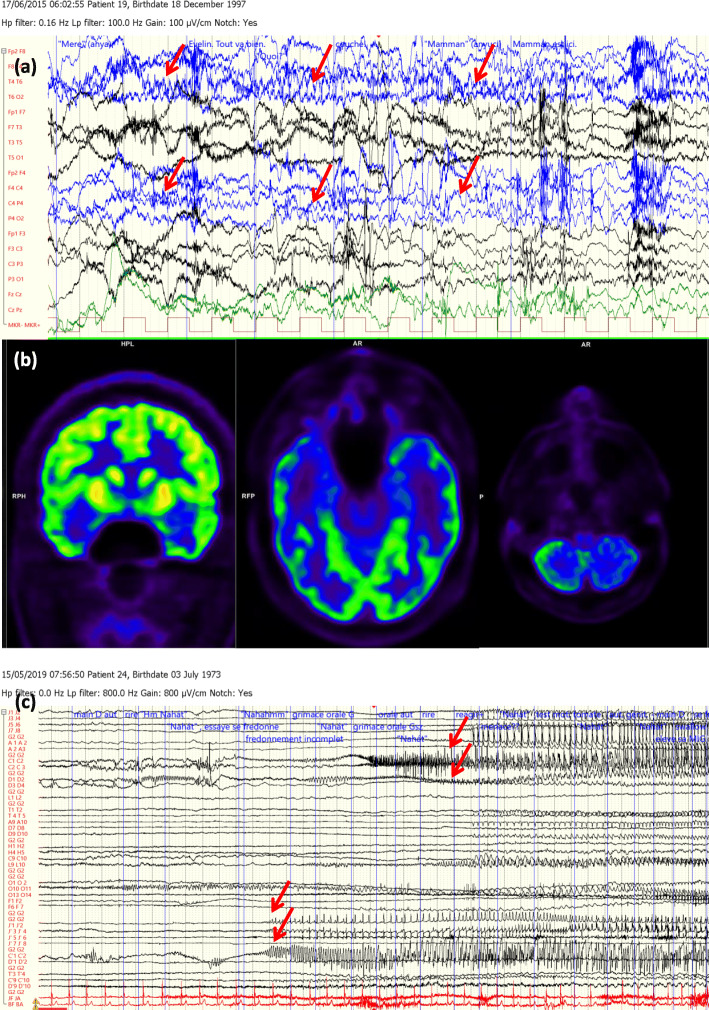
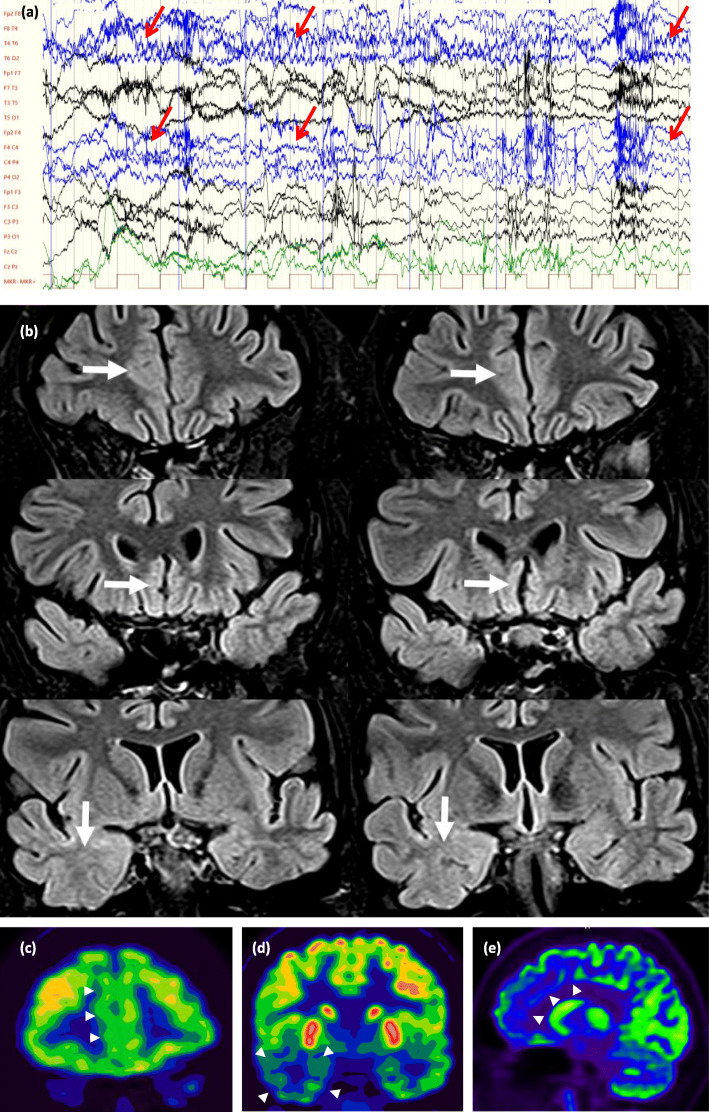
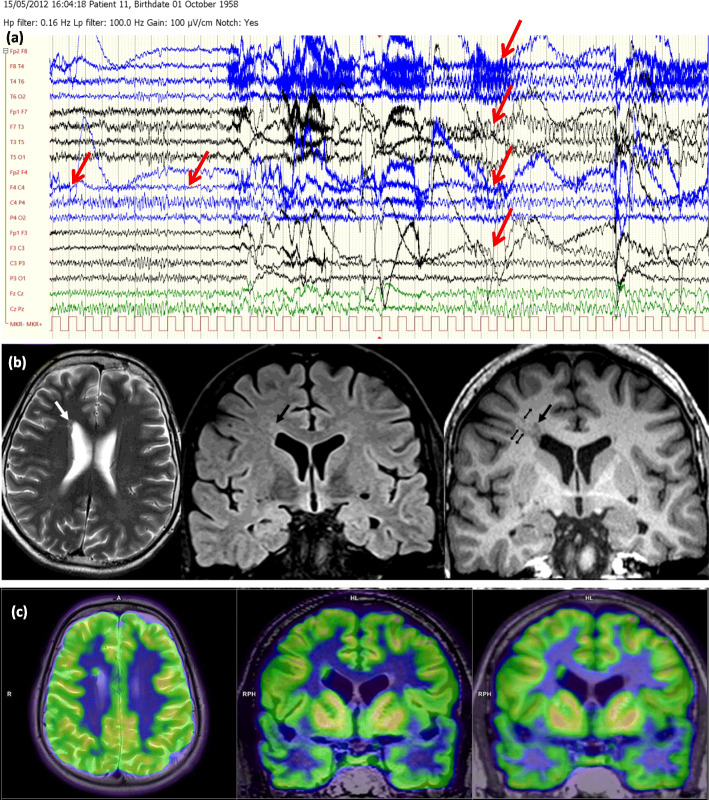
Methods: In a prospective study of patients suffering from drug-resistant focal epilepsy, 30 nonlesional and 30 lesional cases with discordant presurgical results were evaluated using hybrid FDG-PET/MRI.
Results: The hybrid imaging revealed morphological lesion in 18 patients and glucose hypometabolism in 29 patients within the nonlesional group. In the MRI positive group, 4 patients were found to be nonlesional, and in 9 patients at least one more epileptogenic lesion was discovered, while in another 17 cases the original lesion was confirmed by means of hybrid FDG-PET/MRI. As to the therapeutic decision-making, these results helped to indicate resective surgery instead of intracranial EEG (iEEG) monitoring in 2 cases, to avoid any further invasive diagnostic procedures in 7 patients, and to refer 21 patients for iEEG in the nonlesional group. Hybrid FDG-PET/MRI has also significantly changed the original therapeutic plans in the lesional group. Prior to the hybrid imaging, a resective surgery was considered in 3 patients, and iEEG was planned in 27 patients. However, 3 patients became eligible for resective surgery, 6 patients proved to be inoperable instead of iEEG, and 18 cases remained candidates for iEEG due to the hybrid FDG-PET/MRI. Two patients remained candidates for resective surgery and one patient became not eligible for any further invasive intervention.
Conclusions: The results of hybrid FDG-PET/MRI significantly altered the original plans in 19 of 60 cases. The introduction of hybrid FDG-PET/MRI into the presurgical evaluation process had a potential modifying effect on clinical decision-making.
Trial registration: Trial registry: Scientific Research Ethics Committee of the Medical Research Council of Hungary.
Trial registration number: 008899/2016/OTIG . Date of registration: 08 February 2016.
Keywords: Clinical decision-making; Drug-resistant epilepsy; Epilepsy surgery; Hybrid FDG-PET/MRI; Preoperative workflow.
© 2021. The Author(s).
Conflict of interest statement
Neither of the authors has any conflict of interest concerning the materials or methods used in this study or the findings specified in this paper to disclose.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
