Staging tau pathology with tau PET in Alzheimer's disease: a longitudinal study
- PMID: 34537810
- PMCID: PMC8449785
- DOI: 10.1038/s41398-021-01602-5
Staging tau pathology with tau PET in Alzheimer's disease: a longitudinal study
Abstract
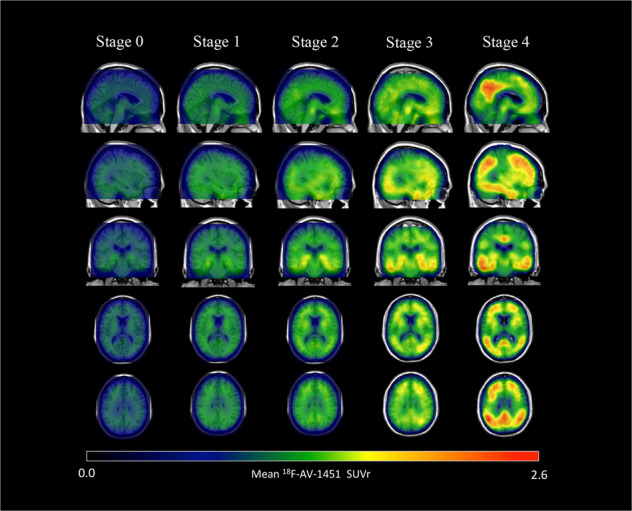
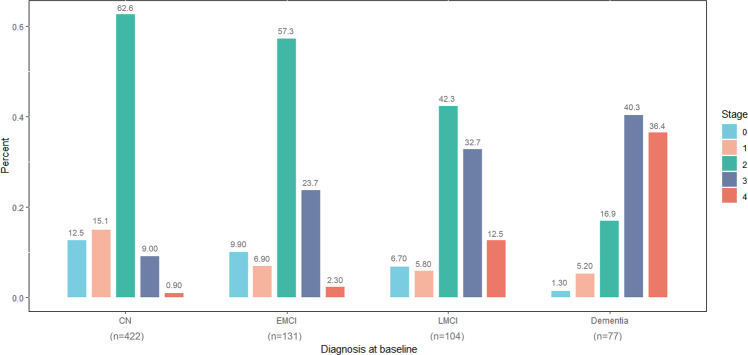
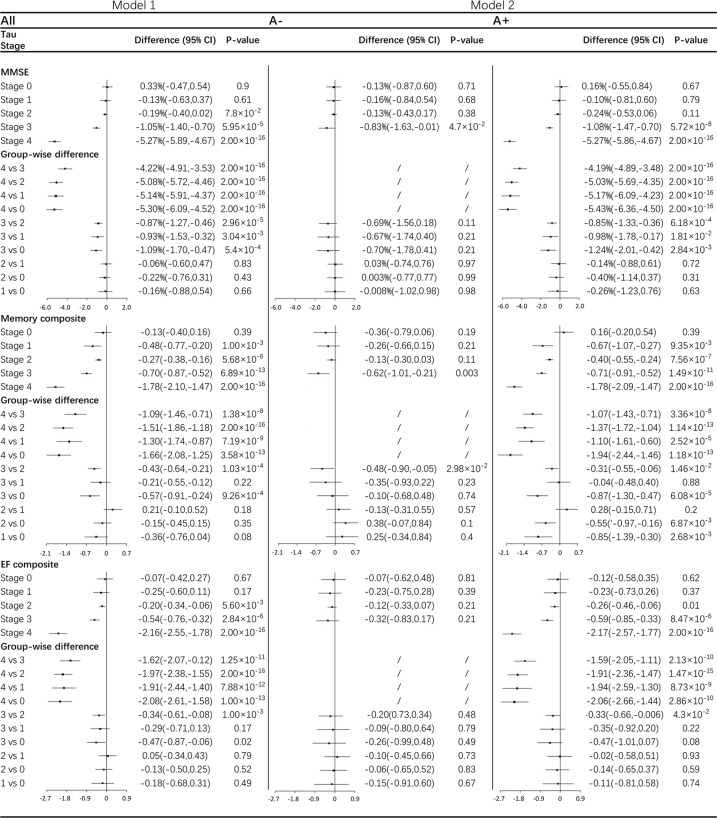
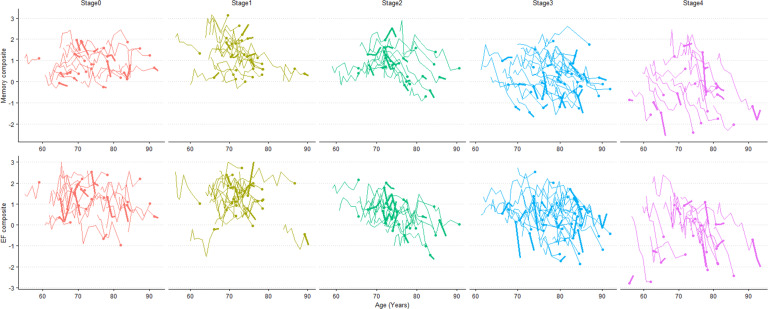
A biological research framework to define Alzheimer' disease with dichotomized biomarker measurement was proposed by National Institute on Aging-Alzheimer's Association (NIA-AA). However, it cannot characterize the hierarchy spreading pattern of tau pathology. To reflect in vivo tau progression using biomarker, we constructed a refined topographic 18F-AV-1451 tau PET staging scheme with longitudinal clinical validation. Seven hundred and thirty-four participants with baseline 18F-AV-1451 tau PET (baseline age 73.9 ± 7.7 years, 375 female) were stratified into five stages by a topographic PET staging scheme. Cognitive trajectories and clinical progression were compared across stages with or without further dichotomy of amyloid status, using linear mixed-effect models and Cox proportional hazard models. Significant cognitive decline was first observed in stage 1 when tau levels only increased in transentorhinal regions. Rates of cognitive decline and clinical progression accelerated from stage 2 to stage 3 and stage 4. Higher stages were also associated with greater CSF phosphorylated tau and total tau concentrations from stage 1. Abnormal tau accumulation did not appear with normal β-amyloid in neocortical regions but prompt cognitive decline by interacting with β-amyloid in temporal regions. Highly accumulated tau in temporal regions independently led to cognitive deterioration. Topographic PET staging scheme have potentials in early diagnosis, predicting disease progression, and studying disease mechanism. Characteristic tau spreading pattern in Alzheimer's disease could be illustrated with biomarker measurement under NIA-AA framework. Clinical-neuroimaging-neuropathological studies in other cohorts are needed to validate these findings.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures