

Apocrine lesions of the breast
- PMID: 34537861
- PMCID: PMC8983539
- DOI: 10.1007/s00428-021-03185-4
Apocrine lesions of the breast
Abstract
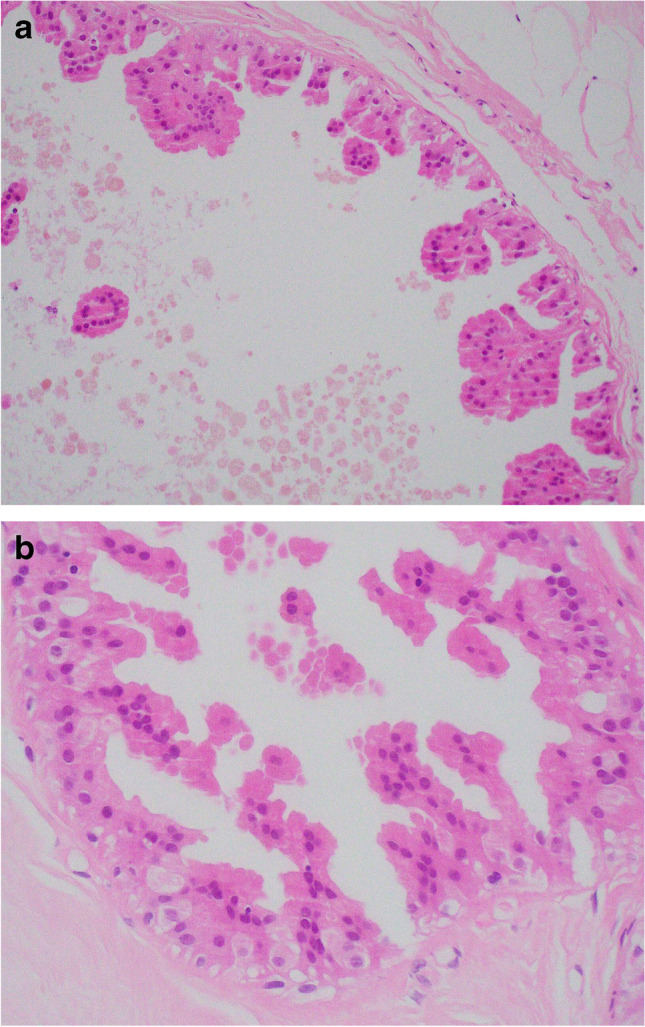
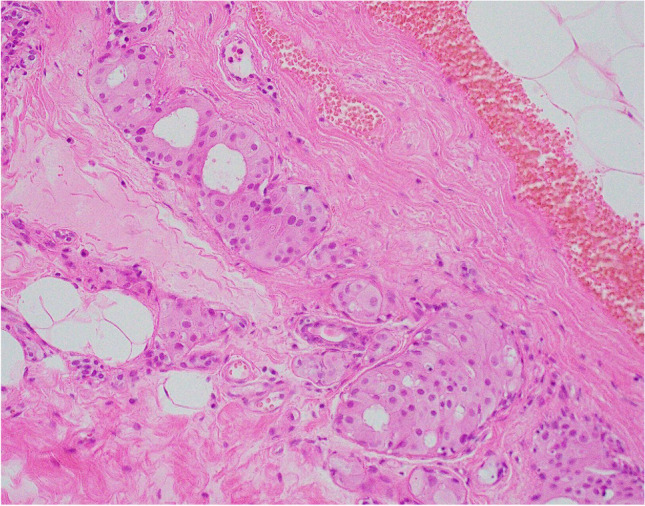
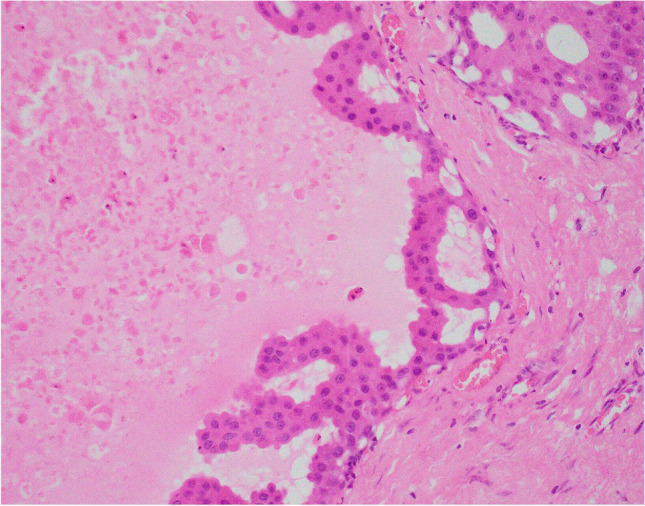
Apocrine change is recognised in benign, atypical and malignant lesions of the breast. Apocrine metaplasia, a frequent finding in the breast of women over the age of 25 years, is most commonly seen in benign cysts with a simple or papillary configuration. Apocrine change is also recognised in other benign lesions including sclerosing adenosis, now known as apocrine adenosis. Apocrine atypia usually refers to cytological atypia in which there is at least threefold variation in nuclear size but architectural atypia may also occur. The distinction between atypical apocrine hyperplasia and non-high-grade apocrine ductal carcinoma in situ may be difficult due to the relative rarity of these entities and the lack of validated diagnostic criteria. Lobular carcinoma in situ (LCIS) with apocrine change is considered to be a variant of pleomorphic LCIS. An apocrine variant of encapsulated papillary carcinoma is also recognised. Apocrine change is described in invasive carcinoma, including no special type, lobular, micropapillary and mucinous variants. The recent WHO 2019 update recognises 'carcinoma with apocrine differentiation' as a special type breast carcinoma based on the presence of apocrine morphology in at least 90% of the tumour. Tumours with apocrine morphology are usually but not always hormone receptor negative. Human epidermal growth factor receptor 2 (HER-2) status is variable. Molecular studies have identified breast tumours with apocrine features and high expression of androgen receptor mRNA including 'luminal androgen receptor tumours' and 'molecular apocrine tumours'. The term 'pure apocrine carcinoma' has been proposed to describe an invasive carcinoma with apocrine morphology that is oestrogen and progesterone receptor negative and androgen receptor positive. HER-2 status may be positive or negative. This article reviews the pathology of benign, atypical and malignant apocrine lesions of the breast, with emphasis on diagnostic criteria including an approach to evaluation of apocrine lesions on needle core biopsy, and recent advances in our understanding of invasive apocrine carcinoma.
Keywords: Apocrine; Atypia; Breast; Carcinoma with apocrine differentiation; In situ carcinoma; Molecular apocrine tumour.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures











References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
