

Efficacy of Vibegron and Mirabegron for Overactive Bladder: A Systematic Literature Review and Indirect Treatment Comparison
- PMID: 34537953
- PMCID: PMC8520873
- DOI: 10.1007/s12325-021-01902-8
Efficacy of Vibegron and Mirabegron for Overactive Bladder: A Systematic Literature Review and Indirect Treatment Comparison
Abstract
Background: In the absence of head-to-head trials, we performed an indirect treatment comparison of the β3-adrenergic agonists vibegron and mirabegron in the treatment of overactive bladder (OAB).
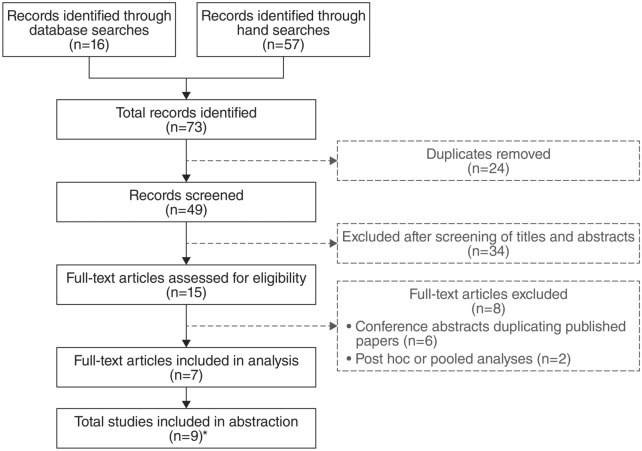
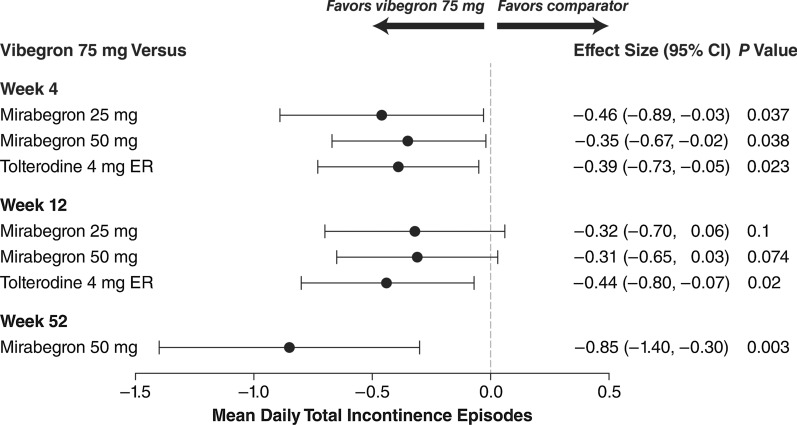
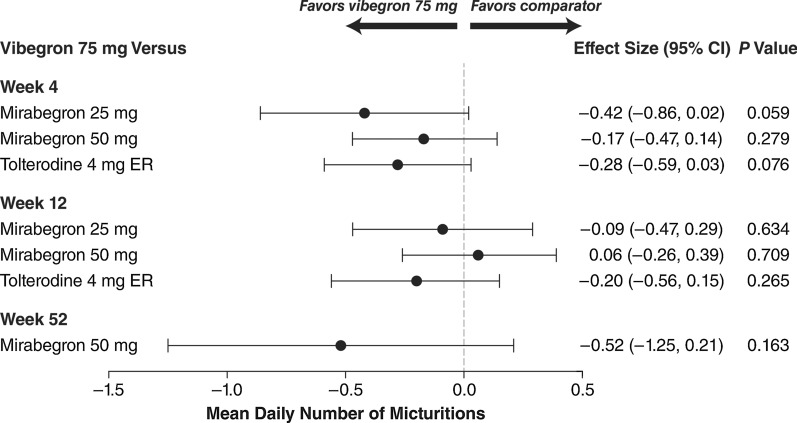
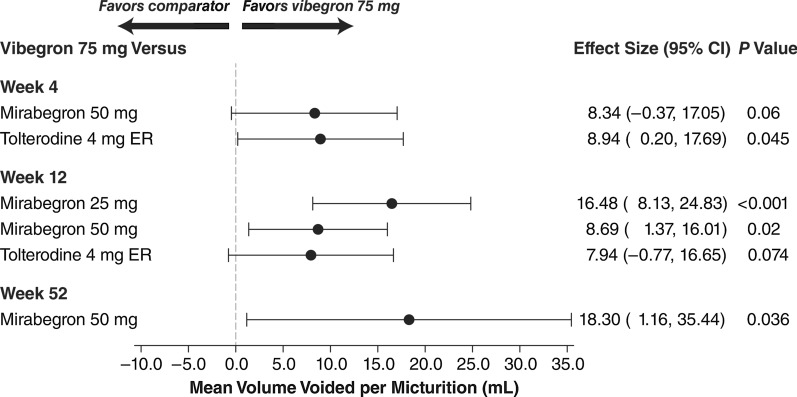
Methods: PubMed, Embase, and Cochrane Library were searched for articles related to phase 3, double-blind, controlled trials of vibegron 75 mg and mirabegron 25/50 mg in patients with OAB. Efficacy outcomes included change from baseline at weeks 4, 12, and 52 in mean daily number of total urinary incontinence episodes and micturitions and mean volume voided/micturition. Effect size was computed as placebo-subtracted change from baseline (weeks 4, 12) or active control (tolterodine)-subtracted change from baseline (week 52) for each treatment group. Adverse events (AEs) are presented descriptively.
Results: After removal of duplicates, 49 records were identified, and after screening 9 met inclusion criteria for analysis. Vibegron showed significantly greater reduction in mean daily number of total incontinence episodes than mirabegron 25 mg at week 4, mirabegron 50 mg (weeks 4, 52), and tolterodine (weeks 4, 12) (P < 0.05, each) and significantly greater improvement in volume voided versus mirabegron 25 mg (week 12), mirabegron 50 mg (weeks 12, 52), and tolterodine (week 4) (P < 0.05, each). Confidence intervals of point estimates overlapped zero for all other comparisons of vibegron and mirabegron (25 or 50 mg) or tolterodine, indicating no significant differences between treatments for these time/endpoints. Urinary tract infection, hypertension, and dry mouth were the most commonly occurring AEs for vibegron, mirabegron, and tolterodine, respectively, in the short-term trials; hypertension was the most commonly occurring AE with all three treatments in the long-term trials.
Conclusions: Vibegron was associated with significant improvement in total incontinence episodes versus mirabegron at 4 and 52 weeks and volume voided at 12 and 52 weeks. Improvement in micturitions was similar between vibegron and mirabegron or tolterodine. Incidence of AEs was generally comparable between vibegron and mirabegron.
Keywords: Adrenergic agonists; Overactive; Urinary bladder; Urinary incontinence.
© 2021. The Author(s).
Figures
References
-
- Gormley EA, Lightner DJ, Burgio KL, et al. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. Linthicum: American Urological Association; 2019. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
