

Wall stresses of early remodeled pulmonary autografts
- PMID: 34538420
- PMCID: PMC8882694
- DOI: 10.1016/j.jtcvs.2021.08.058
Wall stresses of early remodeled pulmonary autografts
Abstract
Objective: The Ross procedure is an excellent option for children or young adults who need aortic valve replacement because it can restore survival to that of the normal aged-matched population. However, autograft remodeling can lead to aneurysmal formation and reoperation, and the biomechanics of this process is unknown. This study investigated postoperative autograft remodeling after the Ross procedure by examining patient-specific autograft wall stresses.
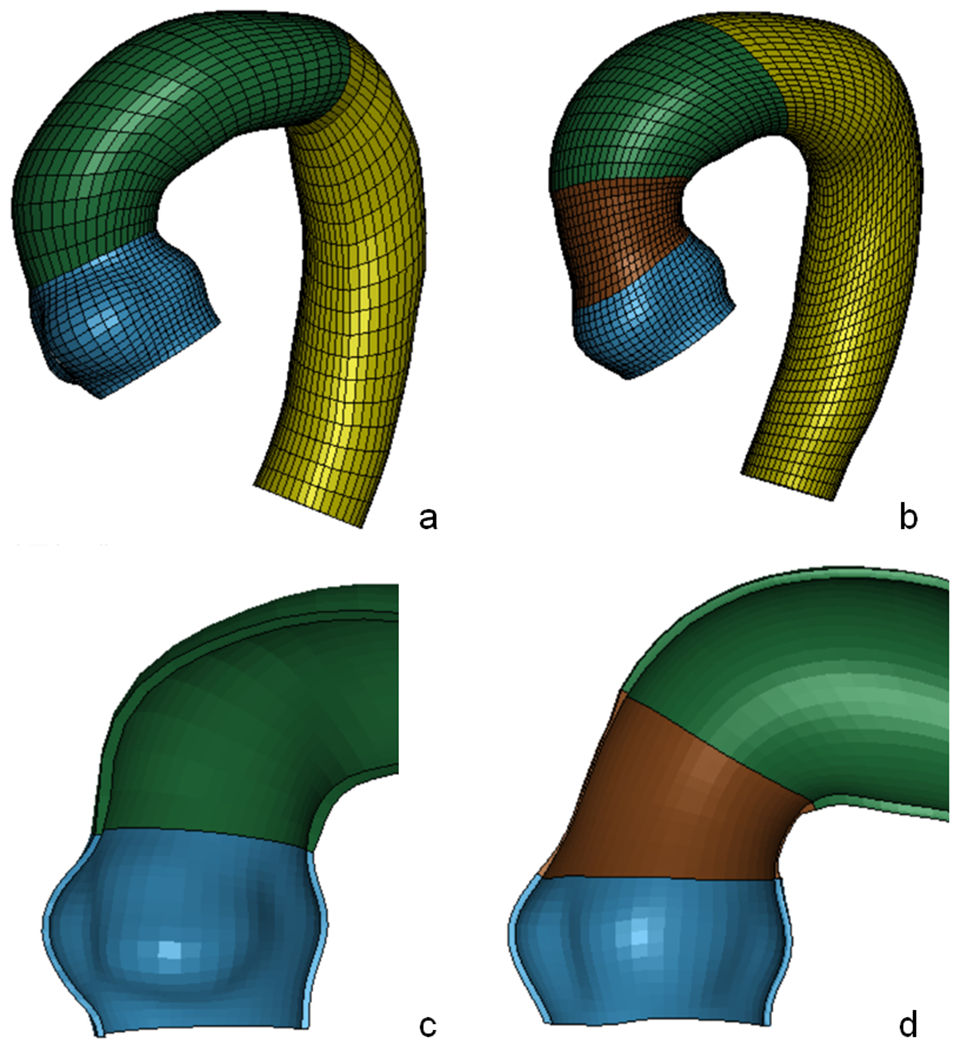
Methods: Patients who have undergone the Ross procedure who had intraoperative pulmonary root and aortic specimens collected were recruited. Patient-specific models (n = 16) were developed using patient-specific material property and their corresponding geometry from cine magnetic resonance imaging at 1-year follow-up. Autograft ± Dacron for aneurysm repair and ascending aortic geometries were reconstructed to develop patient-specific finite element models, which incorporated material properties and wall thickness experimentally measured from biaxial stretching. A multiplicative approach was used to account for prestress geometry from in vivo magnetic resonance imaging. Pressure loading to systemic pressure (120/80) was performed using LS-DYNA software (LSTC Inc, Livermore, Calif).
Results: At systole, first principal stresses were 809 kPa (25%-75% interquartile range, 691-1219 kPa), 567 kPa (485-675 kPa), 637 kPa (555-755 kPa), and 382 kPa (334-413 kPa) at the autograft sinotubular junction, sinuses, annulus, and ascending aorta, respectively. Second principal stresses were 360 kPa (310-426 kPa), 355 kPa (320-394 kPa), 272 kPa (252-319 kPa), and 184 kPa (147-222 kPa) at the autograft sinotubular junction, sinuses, annulus, and ascending aorta, respectively. Mean autograft diameters were 29.9 ± 2.7 mm, 38.3 ± 5.3 mm, and 26.6 ± 4.0 mm at the sinotubular junction, sinuses, and annulus, respectively.
Conclusions: Peak first principal stresses were mainly located at the sinotubular junction, particularly when Dacron reinforcement was used. Patient-specific simulations lay the foundation for predicting autograft dilatation in the future after understanding biomechanical behavior during long-term follow-up.
Keywords: Ross procedure; computational modeling; dilatation; finite element analysis; pulmonary autograft; remodeling; wall stress.
Published by Elsevier Inc.
Conflict of interest statement
Conflicts of Interest: None applicable.
Figures





Comment in
-
Commentary: An opportunity for a new look at the Ross autograft.J Thorac Cardiovasc Surg. 2022 Dec;164(6):1740-1741. doi: 10.1016/j.jtcvs.2021.08.065. Epub 2021 Sep 4. J Thorac Cardiovasc Surg. 2022. PMID: 34521512 No abstract available.
-
Commentary: Biomechanical remodeling of the pulmonary autograft after the Ross procedure.J Thorac Cardiovasc Surg. 2022 Dec;164(6):1739-1740. doi: 10.1016/j.jtcvs.2021.10.043. Epub 2021 Oct 29. J Thorac Cardiovasc Surg. 2022. PMID: 34862059 No abstract available.
References
-
- Laudito A, Brook MM, Suleman S, Bleiweis MS, Thompson LD, Hanley FL and Reddy VM. The Ross procedure in children and young adults: a word of caution. J Thorac Cardiovasc Surg. 2001;122:147–153. - PubMed
-
- Kouchoukos NT, Masetti P, Nickerson NJ, Castner CF, Shannon WD and Davila-Roman VG. The Ross procedure: long-term clinical and echocardiographic follow-up. Ann Thorac Surg. 2004;78:773–81; discussion 773-81. - PubMed
-
- Mastrobuoni S, de Kerchove L, Solari S, Astarci P, Poncelet A, Noirhomme P, Rubay J and El Khoury G. The Ross procedure in young adults: over 20 years of experience in our Institution. Eur J Cardiothorac Surg. 2015;49:507–513. - PubMed
-
- Sievers HH, Stierle U, Charitos EI, Takkenberg JJ, Horer J, Lange R, Franke U, Albert M, Gorski A, Leyh RG, Riso A, Sachweh J, Moritz A, Hetzer R and Hemmer W. A multicentre evaluation of the autograft procedure for young patients undergoing aortic valve replacement: update on the German Ross Registrydagger. Eur J Cardiothorac Surg. 2016;49:212–8. - PubMed
-
- El-Hamamsy I, Eryigit Z, Stevens LM, Sarang Z, George R, Clark L, Melina G, Takkenberg JJ and Yacoub MH. Long-term outcomes after autograft versus homograft aortic root replacement in adults with aortic valve disease: a randomised controlled trial. Lancet. 2010;376:524–31. - PubMed
