

A comprehensive framework for navigating patient care in systemic sclerosis: A global response to the need for improving the practice of diagnostic and preventive strategies in SSc
- PMID: 34538573
- PMCID: PMC8670736
- DOI: 10.1016/j.berh.2021.101707
A comprehensive framework for navigating patient care in systemic sclerosis: A global response to the need for improving the practice of diagnostic and preventive strategies in SSc
Abstract
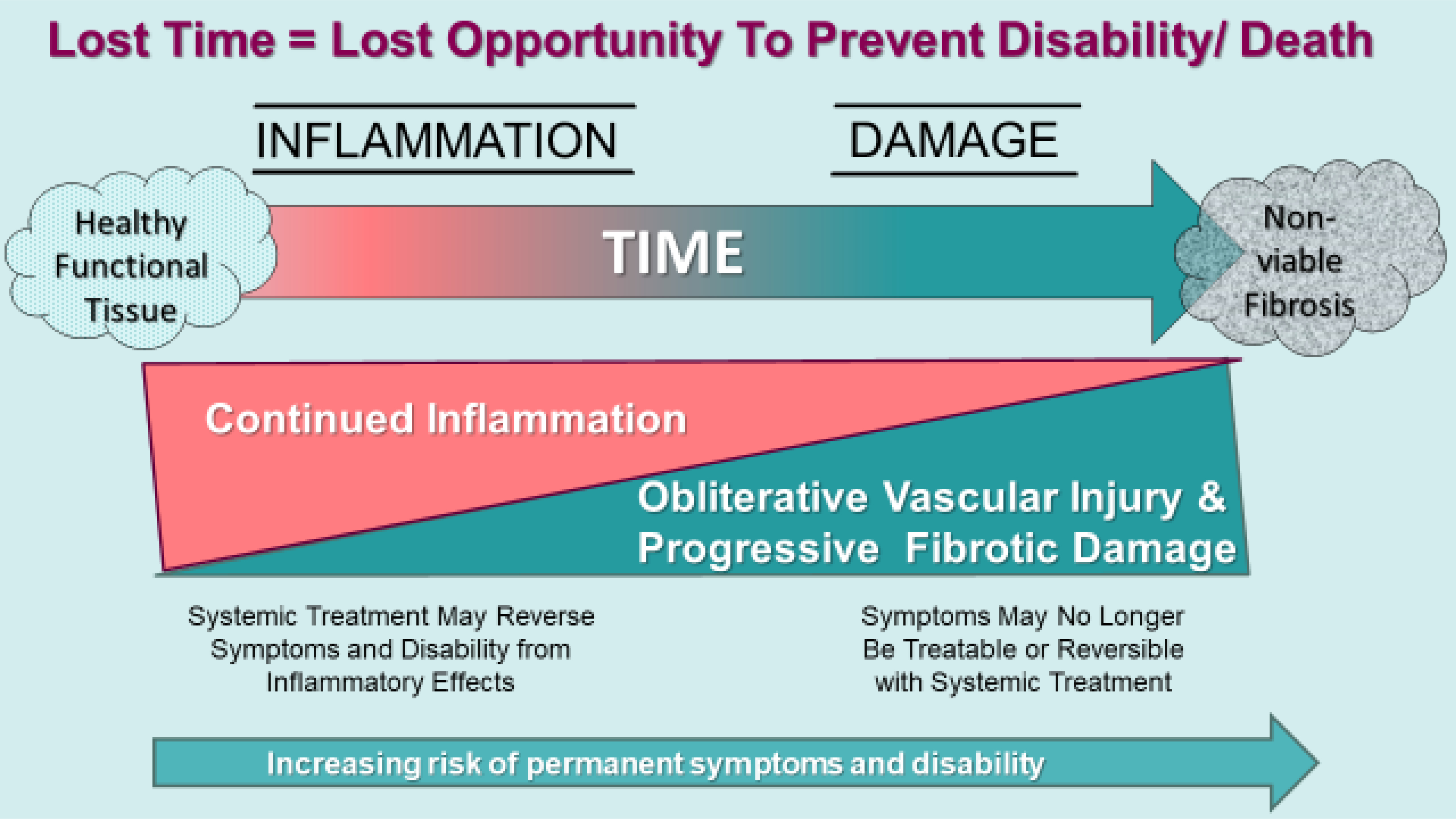
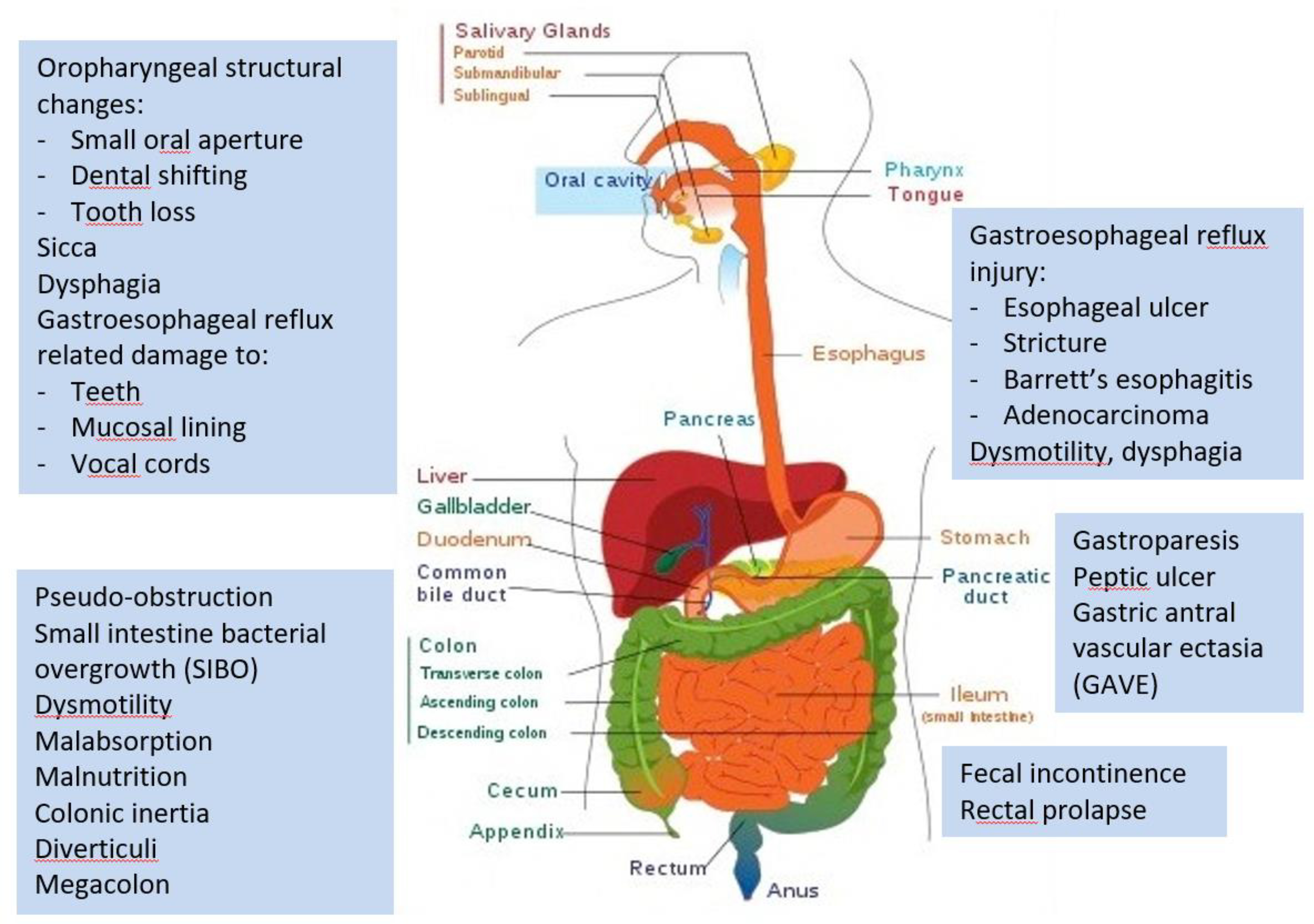
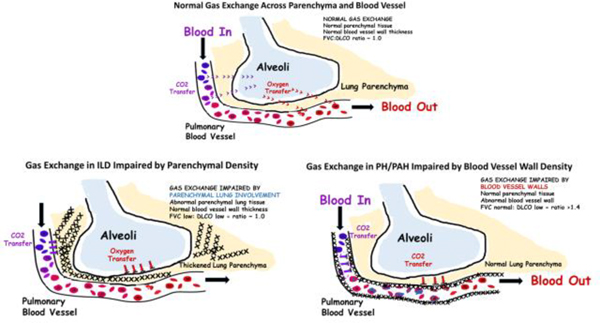
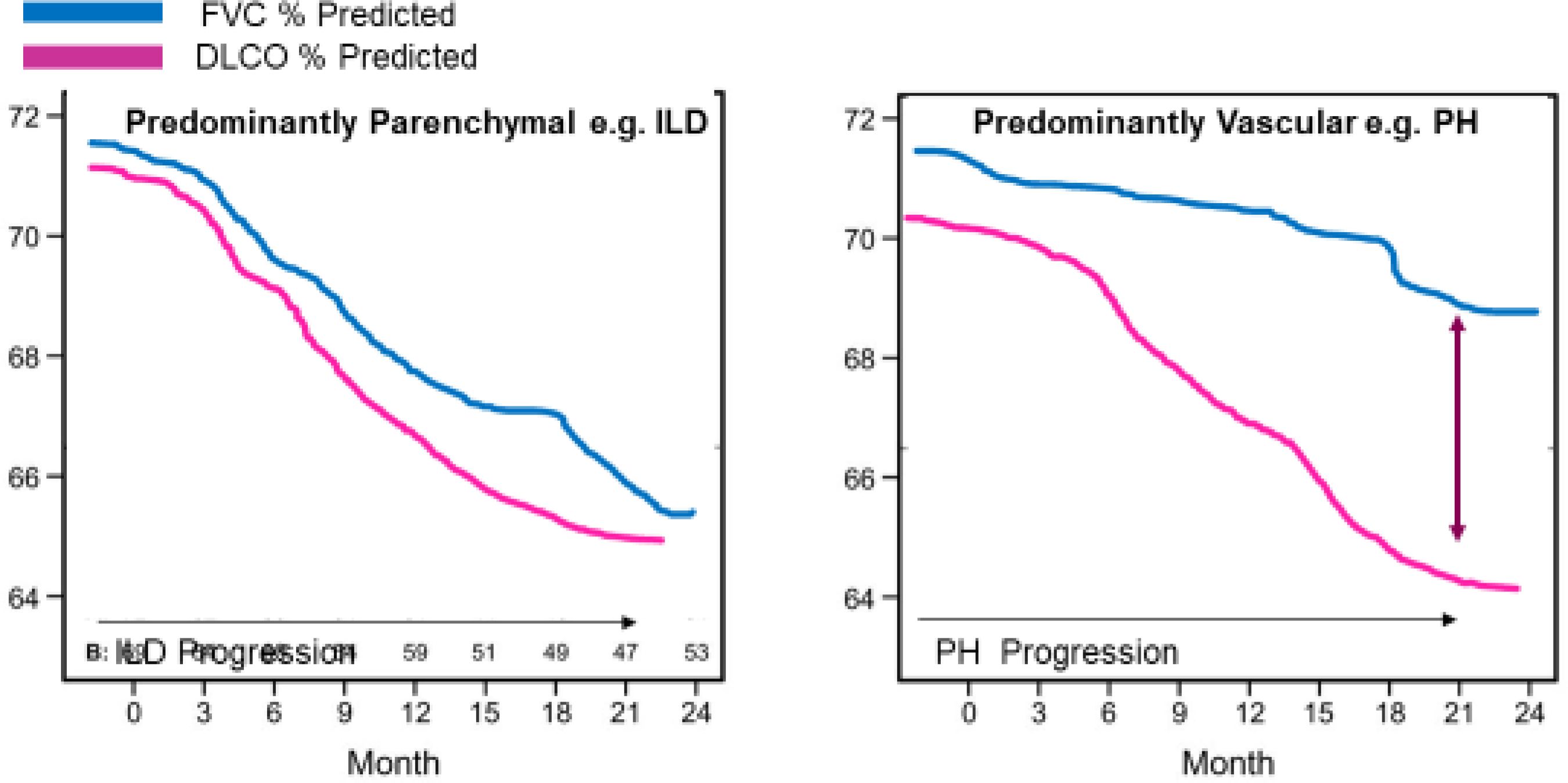
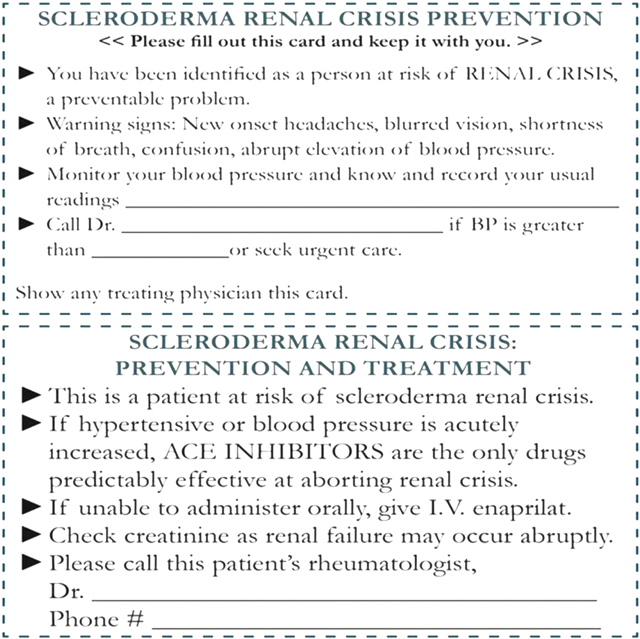
Systemic sclerosis (SSc), the most lethal of rheumatologic conditions, is the cause of death in >50% of SSc cases, led by pulmonary fibrosis followed by pulmonary hypertension and then scleroderma renal crisis (SRC). Multiple other preventable and treatable SSc-related vascular, cardiac, gastrointestinal, nutritional and musculoskeletal complications can lead to disability and death. Vascular injury with subsequent inflammation transforming to irreversible fibrosis and permanent damage characterizes SSc. Organ involvement is often present early in the disease course of SSc, but requires careful history-taking and vigilance in screening to detect. Inflammation is potentially reversible provided that treatment intensity quells inflammation and other immune mechanisms. In any SSc phenotype, opportunities for early treatment are prone to be under-utilized, especially in slowly progressive phenotypes that, in contrast to severe progressive ILD, indolently accrue irreversible organ damage resulting in later-stage life-limiting complications such as pulmonary hypertension, cardiac involvement, and malnutrition. A single SSc patient visit often requires much more physician and staff time, organization, vigilance, and direct management for multiple organ systems compared to other rheumatic or pulmonary diseases. Efficiency and efficacy of comprehensive SSc care enlists trending of symptoms and bio-data. Financial sustainability of SSc care benefits from understanding insurance reimbursement and health system allocation policies for complex patients. Sharing care between recognised SSc centers and local cardiology/pulmonary/rheumatology/gastroenterology colleagues may prevent complications and poor outcomes, while providing support to local specialists. As scleroderma specialists, we offer a practical framework with tools to facilitate an optimal, comprehensive and sustainable approach to SSc care. Improved health outcomes in SSc relies upon recogntion, management and, to the extent possible, prevention of SSc and treatment-related complications.
Keywords: Disability; Interstitial lung disease; Pulmonary fibrosis; Pulmonary hypertension; Quality of life; Renal crisis; Scleroderma; Symptom burden; Systemic sclerosis.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of competing interest None of the authors have conflicts of interest to report that are related to the reported content of this paper.
Figures
References
-
- Gelber AC, Manno RL, Shah AA, et al. Race and association with disease manifestations and mortality in scleroderma: a 20-year experience at the Johns Hopkins Scleroderma Center and review of the literature. Medicine (Baltimore). 2013;92(4):191–205. doi:10.1097/MD.0b013e31829be125 - DOI - PMC - PubMed
-
- Morgan ND, Shah AA, Mayes MD, et al. Clinical and serological features of systemic sclerosis in a multicenter African American cohort: Analysis of the genome research in African American scleroderma patients clinical database. Medicine (Baltimore). 2017;96(51):e8980. doi:10.1097/MD.0000000000008980 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
