

Prognostic factors associated with upper gastrointestinal bleeding based on the French multicenter SANGHRIA trial
- PMID: 34540542
- PMCID: PMC8445676
- DOI: 10.1055/a-1508-5871
Prognostic factors associated with upper gastrointestinal bleeding based on the French multicenter SANGHRIA trial
Abstract
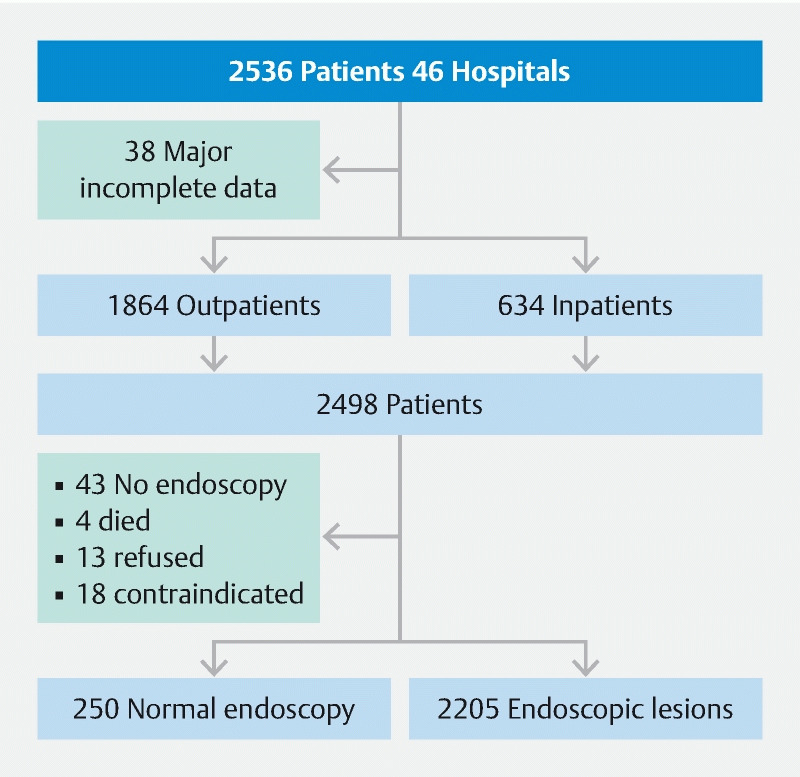
Background and study aims Prognostic and risk factors for upper gastrointestinal bleeding (UGIB) might have changed overtime because of the increased use of direct oral anticoagulants and improved gastroenterological care. This study was undertaken to assess the outcomes of UGIB in light of these new determinants by establishing a new national, multicenter cohort 10 years after the first. Methods Consecutive outpatients and inpatients with UGIB symptoms consulting at 46 French general hospitals were prospectively included between November 2017 and October 2018. They were followed for at least for 6 weeks to assess 6-week rebleeding and mortality rates and factors associated with each event. Results Among the 2498 enrolled patients (mean age 68.5 [16.3] years, 67.1 % men), 74.5 % were outpatients and 21 % had cirrhosis. Median Charlson score was 2 (IQR 1-4) and Rockall score was 5 (IQR 3-6). Within 24 hours, 83.4 % of the patients underwent endoscopy. The main causes of bleeding were peptic ulcers (44.9 %) and portal hypertension (18.9 %). The early in-hospital rebleeding rate was 10.5 %. The 6-week mortality rate was 12.5 %. Predictors significantly associated with 6-week mortality were initial transfusion (OR 1.54; 95 %CI 1.04-2.28), Charlson score > 4 (OR 1.80; 95 %CI 1.31-2.48), Rockall score > 5 (OR 1.98; 95 %CI 1.39-2.80), being an inpatient (OR 2.45; 95 %CI 1.76-3.41) and rebleeding (OR 2.6; 95 %CI 1.85-3.64). Anticoagulant therapy was not associated with dreaded outcomes. Conclusions The 6-week mortality rate remained high after UGIB, especially for inpatients. Predictors of mortality underlined the weight of comorbidities on outcomes.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Competing interests Dr. Nahon has received lecture fees from MSD, Takeda and Sandoz, and consulting fees from MSD, Takeda, Janssen, Sandoz, Ferring, and Vifor. Dr. Arotcarena has received funds from Gilead and Abbvie to attend meetings. Dr. Macaigne has received funding from Jansen, Takeda, Abbvie, and Tillots to attend meetings.
References
-
- Gralnek I, Dumonceau J-M, Kuipers E et al.Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2015;47:a1–46. - PubMed
-
- Hwang J H, Fisher D A, Ben-Menachem T et al.The role of endoscopy in the management of acute non-variceal upper GI bleeding. Gastrointest Endosc. 2012;75:1132–1138. - PubMed
-
- Hwang J H, Shergill A K, Acosta R D et al.The role of endoscopy in the management of variceal hemorrhage. Gastrointest Endosc. 2014;80:221–227. - PubMed
-
- de Franchis R. Expanding consensus in portal hypertension. J Hepatol. 2015;63:743–752. - PubMed
-
- Sey M SL, Mohammed S B, Brahmania M et al.Comparative outcomes in patients with ulcer- vs non-ulcer-related acute upper gastrointestinal bleeding in the United Kingdom: a nationwide cohort of 4474 patients. Aliment Pharmacol Ther. 2019;49:537–545. - PubMed
LinkOut - more resources
Full Text Sources