

Colon capsule endoscopy in clinical practice: lessons from a national 5-year observational prospective cohort
- PMID: 34540548
- PMCID: PMC8445686
- DOI: 10.1055/a-1526-0923
Colon capsule endoscopy in clinical practice: lessons from a national 5-year observational prospective cohort
Abstract
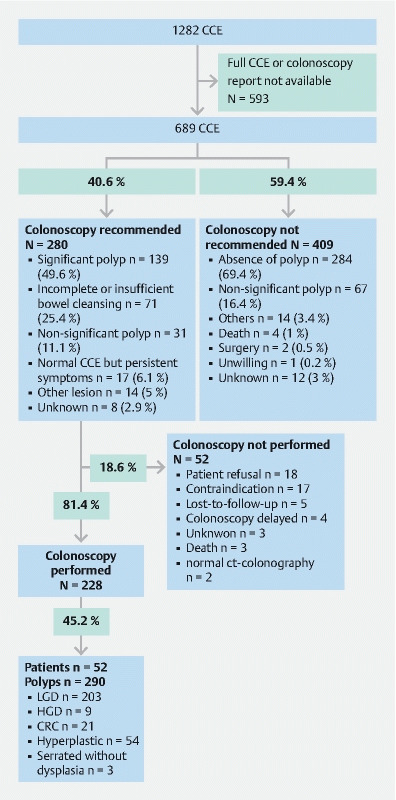
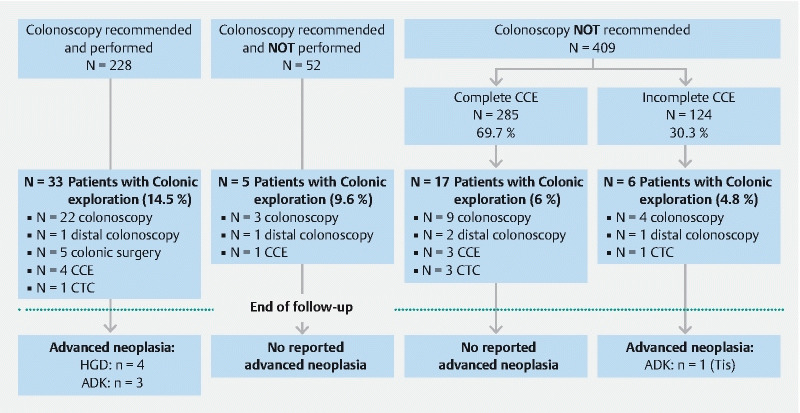
Background and study aims Colon capsule endoscopy (CCE) has been proposed as an alternative to colonoscopy for screening patients at average risk of colorectal cancer (CRC). A prospective national cohort was developed to assess relevance of CCE in real-life practice and its short- and long-term impacts on clinical management. Patients and methods All patients who underwent a CCE in France were prospectively enrolled from January 2011 to May 2016 and reached annually by phone until May 2017. All CCE and colonoscopy reports were systematically collected. Results During the study period, 689 CCEs were analyzed from 14 medical centers. Median follow-up time was 35 months [IQR: 12-50]. Indication for CCE was mainly for elderly patients (median age: 70 years, IQR: [61-79]) due to anesthetic or colonoscopy contraindication (n = 307; 44.6 %). Only 337 CCEs (48.9 %) were both complete and with adequate bowel preparation. Advanced neoplasia (adenoma with high-grade dysplasia or CRC) was diagnosed following 32 CCEs (4.6 %). Among patients who underwent colonoscopy or therapeutic surgery following CCE, 18.8 % of all advanced neoplasias (6/32) had not been diagnosed by CCE mainly due to technical issues. Performing a colonoscopy in the case of significant polyps or insufficient bowel cleansing or after an incomplete CCE allowed the diagnosis of 96.9 % of all identified advanced neoplasias (31/32). Conclusions Outside the scope of academic trials, improvement is needed to increase the reliability of CCE as less than half were considered optimal i. e. complete with adequate bowel cleansing. Most of missed colonic advanced neoplasia were due to incomplete CCE with distal neoplasia location.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Competing interests Dr. Benech has received a travel grant from Maat. R. Benzmouzig has received research support from Medtronic, is a consultant for Medtronic and Alfasigma, has taught for Medtronic and Mayoly Spindler, and received a Congress invitation from Mayoly Spindler. Dr. Ponchon has taught for Olympus. Dr. Dray has received research support from MSD and Norgine, done consulting for Medtronic and Boston Scientific, taught for Fujifilm, Medtronic, Alfasigma, and Bouchara-Recordati, received a Congress invitation from AbbVie, Biocodex, Boston Scientific, Hospira (groupe Pfizer), and MSD, and is a cofounder of and shareholder in Augmented Endoscopy. Dr. Sacher-Huvelin has done consulting for Medtronic. Dr. Galmiche has done consulting for Medtronic and Fujifilm. Dr. Saurin has done consulting for AbbVie, Bouchara-Recordati, Mayoly Spindler, Medtronic, ABS-Bolton, and Intromedic and received a Congress invitation from AbbVie, MSD, and Hospira (groupe Pfizer). This study was funded by Medtronic, which provided CCE, funds for e-CRF constitution, and salary for a clinical research assistant that reviewed all CCE, colonoscopy reports, and performed the follow-up.
Figures
Comment in
-
Real-life practice data on colon capsule endoscopy: We need them fast!Endosc Int Open. 2022 Mar 14;10(3):E230-E231. doi: 10.1055/a-1728-9371. eCollection 2022 Mar. Endosc Int Open. 2022. PMID: 35295244 Free PMC article. No abstract available.
References
-
- Winawer S J, Zauber A G, Ho M N et al.Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med. 1993;329:1977–1981. - PubMed
-
- Wolf A MD, Fontham E TH, Church T R et al.Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J Clin. 2018;68:250–281. - PubMed
-
- Rembacken B, Hassan C, Riemann J F et al.Quality in screening colonoscopy: position statement of the European Society of Gastrointestinal Endoscopy (ESGE) Endoscopy. 2012;44:957–968. - PubMed
-
- Eliakim R, Fireman Z, Gralnek I M et al.Evaluation of the PillCam Colon capsule in the detection of colonic pathology: results of the first multicenter, prospective, comparative study. Endoscopy. 2006;38:963–970. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources