

Trauma Scores and Their Prognostic Value for the Outcome Following Pediatric Polytrauma
- PMID: 34540770
- PMCID: PMC8446435
- DOI: 10.3389/fped.2021.721585
Trauma Scores and Their Prognostic Value for the Outcome Following Pediatric Polytrauma
Abstract
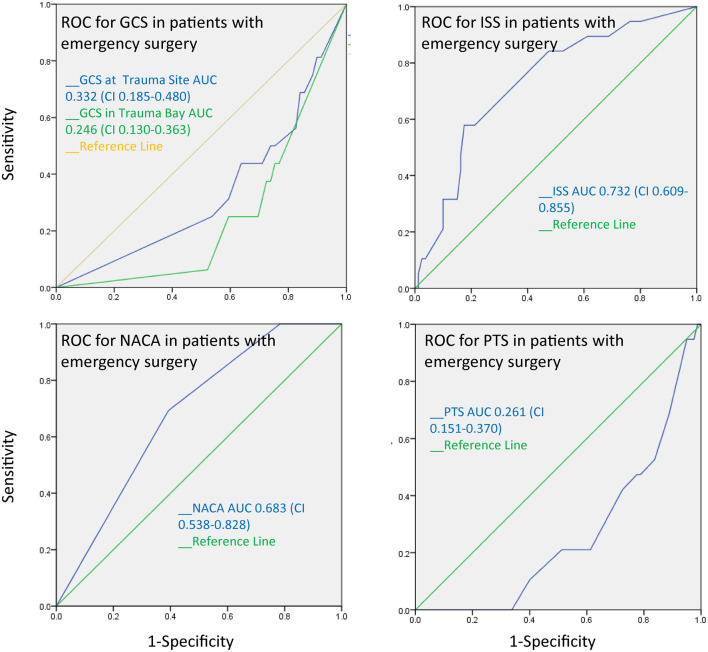
Purpose: The management and prognostic assessment of pediatric polytrauma patients can pose substantial challenges. Trauma scores developed for adults are not universally applicable in children. An accurate prediction of the severity of trauma and correct assessment of the necessity of surgical procedures are important for optimal treatment. Several trauma scores are currently available, but the advantages and drawbacks for use in pediatric patients are unclear. This study examines the value of the trauma scores Injury Severity Score (ISS), Pediatric Trauma Score (PTS), National Advisory Committee for Aeronautics (NACA), and Glasgow Coma Score (GCS) for the assessment of the polytraumatized child. Methods: In a retrospective study, 97 patients aged 0-17 years who presented with polytrauma and an ISS ≥16 in the trauma bay were included in the study. Patient records including radiological studies were analyzed. Pathological imaging findings and emergency surgery were assessed as outcome variables and the predictive value of the trauma scores were analyzed using receiver operator characteristic (ROC) curves. Statistical significance was set at an alpha level of P ≤ 0.05. Results: In this study, 35 of the 97 studied children had pathological cranial computed findings. These either underwent craniectomy or trepanation or a parenchymal catheter was placed for intracranial pressure monitoring. Abdominal trauma was present in 45 patients, 16 of which were treated surgically. Forty-three patients arrived with thoracic injuries, 10 of which received a thoracic drainage. One child underwent an emergency thoracotomy. Predictive accuracy for emergency surgery calculated using receiver-operator characteristic (ROC) curves was highest for ISS and NACA scores (0,732 and 0.683, respectively), and lower for GCS (0.246) and PTS (0.261). Conclusion: In our study cohort, initial ISS and NACA scores better predicted operative interventions and outcome than PTS or GCS for polytraumatized pediatric patients.
Keywords: glasgow coma scale; injury severity score; national advisory committee for aeronautics; outcome; pediatric polytrauma; pediatric trauma score.
Copyright © 2021 Wendling-Keim, Hefele, Muensterer and Lehner.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- Lehner M, Hoffmann F, Kammer B, Heinrich M, Falkenthal L, Wendling-Keim D, Kurz M. Reduction of treatment time for children in the trauma room care: impact of implementation of an interdisciplinary trauma room concept (iTRAPS). Anaesthesist. (2018) 67:914–21. 10.1007/s00101-018-0500-z - DOI - PubMed
-
- Brown J, Meigh M. Calculated decisions: pediatric Glasgow coma scale. Pediatr Emerg Med Practice. (2018) 15(Suppl.6):CD1–2. - PubMed
-
- Runde D. Calculated decisions: Glasgow coma scale. Emerg Med Practice. (2018) 20(Suppl.10):CD4–6. - PubMed
LinkOut - more resources
Full Text Sources