

Removing Well-Fixed, Collared and Noncollared Tapered Hip Stems Without an Extended Trochanteric Osteotomy Using a Novel Stem Removal System
- PMID: 34541268
- PMCID: PMC8435937
- DOI: 10.1016/j.artd.2021.07.004
Removing Well-Fixed, Collared and Noncollared Tapered Hip Stems Without an Extended Trochanteric Osteotomy Using a Novel Stem Removal System
Abstract
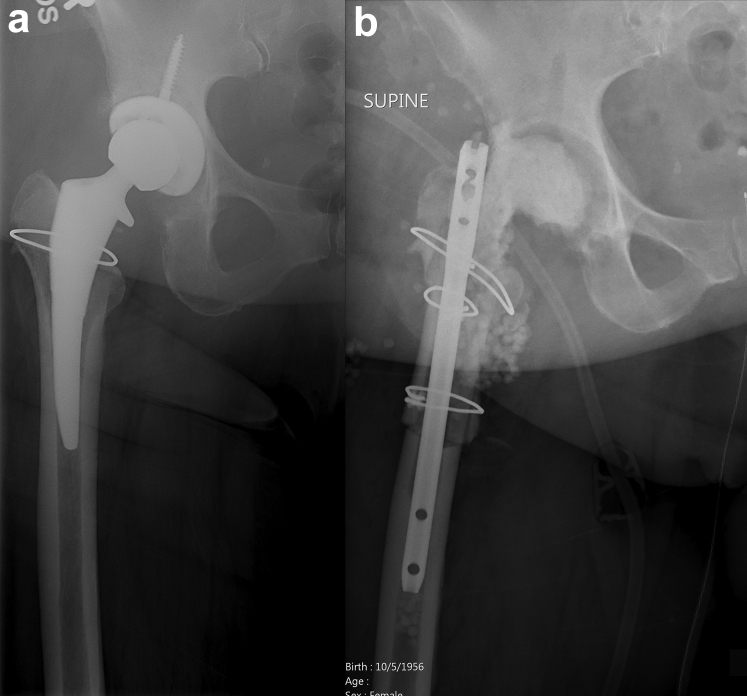
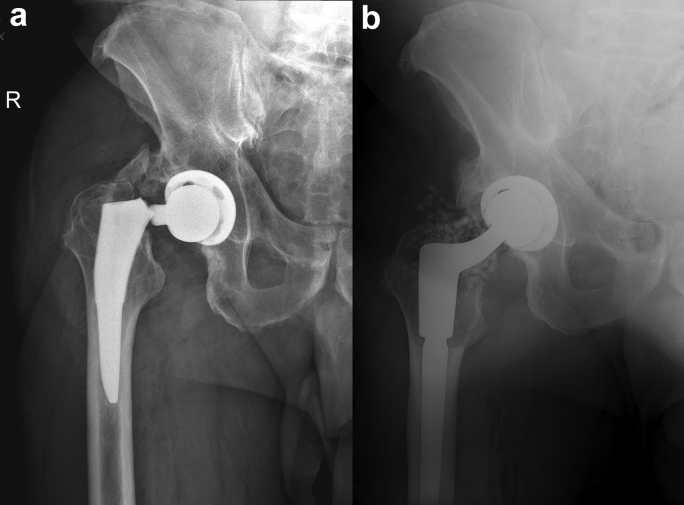
Improvements in materials, components, and surgical techniques in cementless total hip arthroplasty are resulting in improved femoral stem fixation through bony ongrowth or ingrowth. While improved femoral stem fixation is one reason for the current excellent total hip survivorship, indications for stem removal such as infection, implant fracture, or osteolysis remain. A commonly used technique for fully ingrown femoral stems is an extended trochanteric osteotomy which can result in comminuted fractures of the proximal femur during stem removal requiring additional fixation. Therefore, a novel hip stem removal was developed to facilitate removal of these well-ingrown stems without the need for an extended trochanteric osteotomy. This study describes the removal system and surgical technique and presents a case series of successfully removed ingrown stems.
Keywords: Cementless; Explantation; Femoral stem removal; Resection arthroplasty; Revision hip arthroplasty.
© 2021 The Authors.
Figures






References
-
- Kurtz S., Ong K., Lau E., Mowat F., Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780. - PubMed
-
- Brown J.M., Mistry J.B., Cherian J.J. Femoral component revision of total hip arthroplasty. Orthopedics (Online) 2016;39(6):e1129. - PubMed
-
- Aribindi R., Paprosky W., Nourbash P., Kronick J., Barba M. Extended proximal femoral osteotomy. Instr Course Lect. 1999;48:19. - PubMed
-
- Miner T.M., Momberger N.G., Chong D., Paprosky W.L. The extended trochanteric osteotomy in revision hip arthroplasty: a critical review of 166 cases at mean 3-year, 9-month follow-up. J Arthroplasty. 2001;16(8 Suppl 1):188. - PubMed
-
- Huffman G.R., Ries M.D. Combined vertical and horizontal cable fixation of an extended trochanteric osteotomy site. J Bone Joint Surg Am. 2003;85(2):273. - PubMed
LinkOut - more resources
Full Text Sources
