

Predictors of functional outcomes in patients with facioscapulohumeral muscular dystrophy
- PMID: 34542603
- PMCID: PMC8677548
- DOI: 10.1093/brain/awab326
Predictors of functional outcomes in patients with facioscapulohumeral muscular dystrophy
Abstract
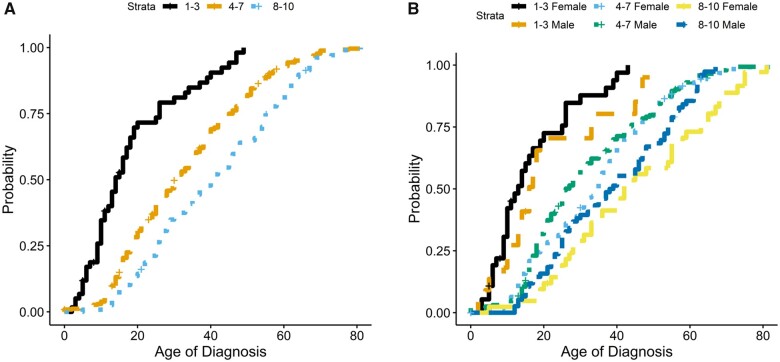
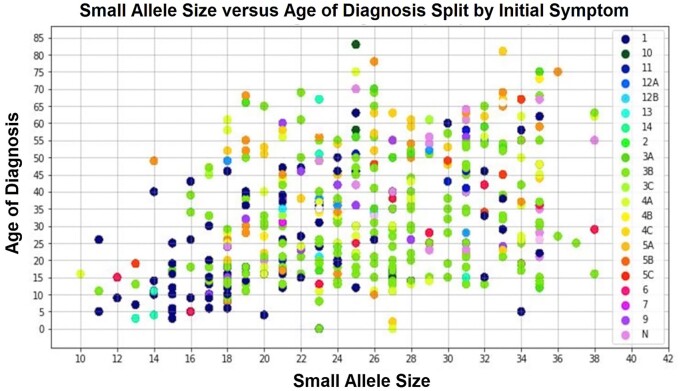
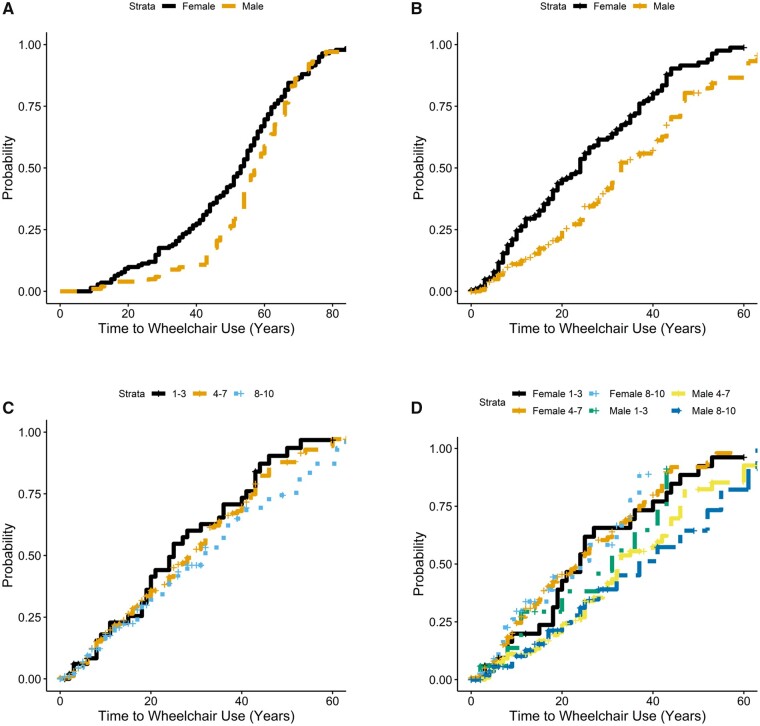
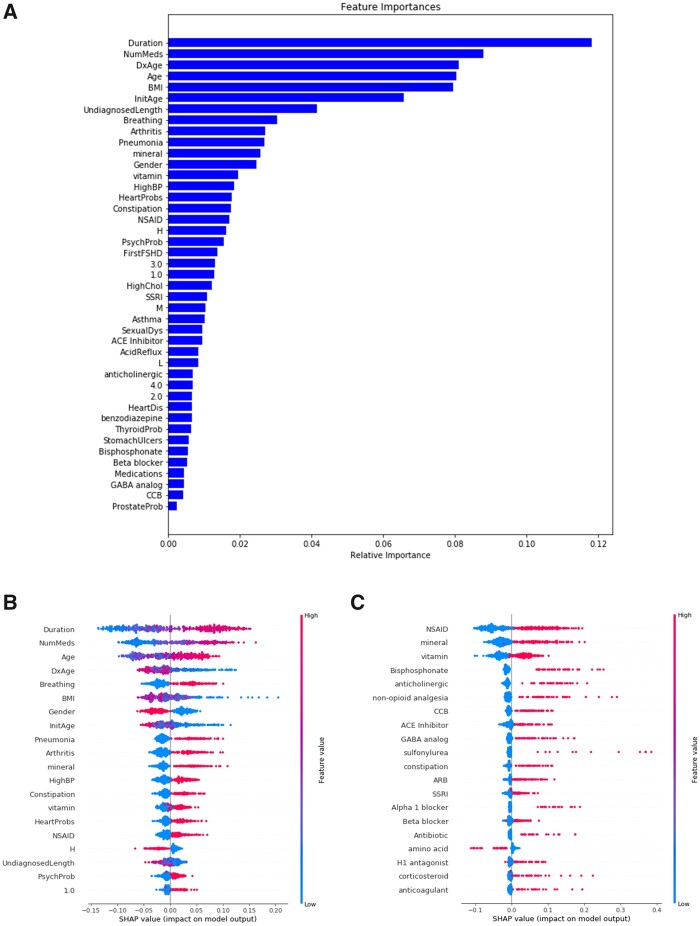
Facioscapulohumeral muscular dystrophy (FSHD) is one of the most prevalent muscular dystrophies characterized by considerable variability in severity, rates of progression and functional outcomes. Few studies follow FSHD cohorts long enough to understand predictors of disease progression and functional outcomes, creating gaps in our understanding, which impacts clinical care and the design of clinical trials. Efforts to identify molecularly targeted therapies create a need to better understand disease characteristics with predictive value to help refine clinical trial strategies and understand trial outcomes. Here we analysed a prospective cohort from a large, longitudinally followed registry of patients with FSHD in the USA to determine predictors of outcomes such as need for wheelchair use. This study analysed de-identified data from 578 individuals with confirmed FSHD type 1 enrolled in the United States National Registry for FSHD Patients and Family members. Data were collected from January 2002 to September 2019 and included an average of 9 years (range 0-18) of follow-up surveys. Data were analysed using descriptive epidemiological techniques, and risk of wheelchair use was determined using Cox proportional hazards models. Supervised machine learning analysis was completed using Random Forest modelling and included all 189 unique features collected from registry questionnaires. A separate medications-only model was created that included 359 unique medications reported by participants. Here we show that smaller allele sizes were predictive of earlier age at onset, diagnosis and likelihood of wheelchair use. Additionally, we show that females were more likely overall to progress to wheelchair use and at a faster rate as compared to males, independent of genetics. Use of machine learning models that included all reported clinical features showed that the effect of allele size on progression to wheelchair use is small compared to disease duration, which may be important to consider in trial design. Medical comorbidities and medication use add to the risk for need for wheelchair dependence, raising the possibility for better medical management impacting outcomes in FSHD. The findings in this study will require further validation in additional, larger datasets but could have implications for clinical care, and inclusion criteria for future clinical trials in FSHD.
Keywords: artificial intelligence; facioscapulohumeral muscular dystrophy; functional outcomes; machine learning; wheelchair use.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Random forest: random results or meaningful insights for patients with facioscapulohumeral muscular dystrophy?Brain. 2021 Dec 16;144(11):3288-3290. doi: 10.1093/brain/awab389. Brain. 2021. PMID: 34636841 Free PMC article.
References
-
- Flanigan KM, Coffeen CM, Sexton L, Stauffer D, Brunner S, Leppert MF.. Genetic characterization of a large, historically significant Utah kindred with facioscapulohumeral dystrophy. Neuromuscul Disord. 2001;11(6-7):525–529. - PubMed
-
- Mostacciuolo ML, Pastorello E, Vazza G, et al.Facioscapulohumeral muscular dystrophy: Epidemiological and molecular study in a north-east Italian population sample. Clin Genet. 2009;75(6):550–555. - PubMed
-
- Padberg GW, Frants RR, Brouwer OF, Wijmenga C, Bakker E, Sandkuijl LA.. Facioscapulohumeral muscular dystrophy in the Dutch population. Muscle Nerve Suppl. 1995;2(2):S81–S84. - PubMed
-
- Banerji CRS, Cammish P, Evangelista T, Zammit PS, Straub V, Marini-Bettolo C.. Facioscapulohumeral muscular dystrophy 1 patients participating in the UK FSHD registry can be subdivided into 4 patterns of self-reported symptoms. Neuromuscul Disord. 2020;30(4):315–328. - PubMed
