

Interventions to Reduce Hospital Length of Stay in High-risk Populations: A Systematic Review
- PMID: 34542615
- PMCID: PMC8453321
- DOI: 10.1001/jamanetworkopen.2021.25846
Interventions to Reduce Hospital Length of Stay in High-risk Populations: A Systematic Review
Abstract
Importance: Many strategies to reduce hospital length of stay (LOS) have been implemented, but few studies have evaluated hospital-led interventions focused on high-risk populations. The Agency for Healthcare Research and Quality (AHRQ) Learning Health System panel commissioned this study to further evaluate system-level interventions for LOS reduction.
Objective: To identify and synthesize evidence regarding potential systems-level strategies to reduce LOS for patients at high risk for prolonged LOS.
Evidence review: Multiple databases, including MEDLINE and Embase, were searched for English-language systematic reviews from January 1, 2010, through September 30, 2020, with updated searches through January 19, 2021. The scope of the protocol was determined with input from AHRQ Key Informants. Systematic reviews were included if they reported on hospital-led interventions intended to decrease LOS for high-risk populations, defined as those with high-risk medical conditions or socioeconomically vulnerable populations (eg, patients with high levels of socioeconomic risk, who are medically uninsured or underinsured, with limited English proficiency, or who are hospitalized at a safety-net, tertiary, or quaternary care institution). Exclusion criteria included interventions that were conducted outside of the hospital setting, including community health programs. Data extraction was conducted independently, with extraction of strength of evidence (SOE) ratings provided by systematic reviews; if unavailable, SOE was assessed using the AHRQ Evidence-Based Practice Center methods guide.
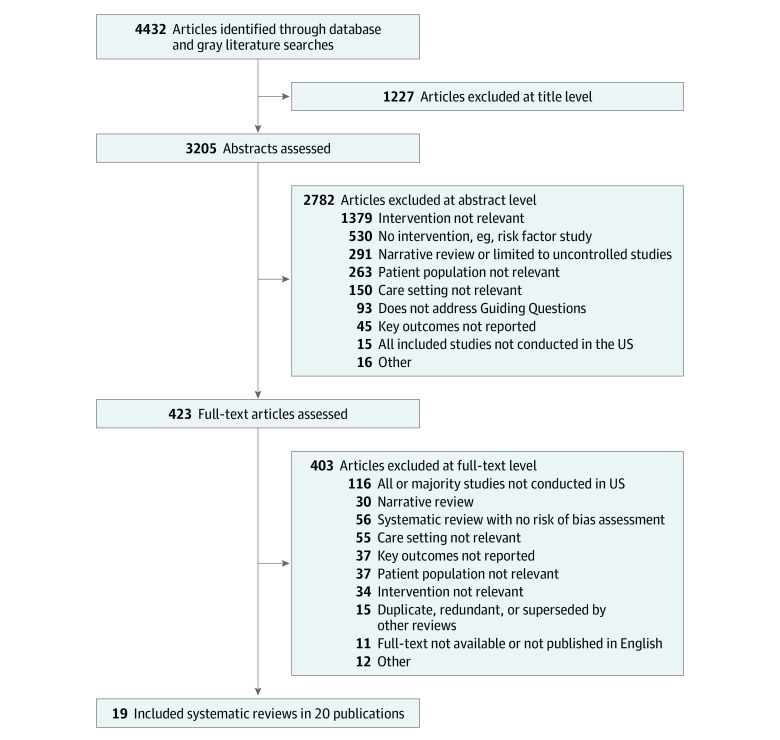
Findings: Our searches yielded 4432 potential studies. We included 19 systematic reviews reported in 20 articles. The reviews described 8 strategies for reducing LOS in high-risk populations: discharge planning, geriatric assessment, medication management, clinical pathways, interdisciplinary or multidisciplinary care, case management, hospitalist services, and telehealth. Interventions were most frequently designed for older patients, often those who were frail (9 studies), or patients with heart failure. There were notable evidence gaps, as there were no systematic reviews studying interventions for patients with socioeconomic risk. For patients with medically complex conditions, discharge planning, medication management, and interdisciplinary care teams were associated with inconsistent outcomes (LOS, readmissions, mortality) across populations. For patients with heart failure, clinical pathways and case management were associated with reduced length of stay (clinical pathways: mean difference reduction, 1.89 [95% CI, 1.33 to 2.44] days; case management: mean difference reduction, 1.28 [95% CI, 0.52 to 2.04] days).
Conclusions and relevance: This systematic review found inconsistent results across all high-risk populations on the effectiveness associated with interventions, such as discharge planning, that are often widely used by health systems. This systematic review highlights important evidence gaps, such as the lack of existing systematic reviews focused on patients with socioeconomic risk factors, and the need for further research.
Conflict of interest statement
Figures
References
-
- McDermott KW, Elixhauser A, Sun R. Trends in hospital inpatient stays in the United States, 2005–2014. HCUP Statistical Brief #225. Agency for Healthcare Research and Quality; 2017:18.
