

Outcome of ductus arteriosus stenting including vertical tubular and convoluted tortuous ducts with emphasis on technical considerations
- PMID: 34542737
- PMCID: PMC8452800
- DOI: 10.1186/s43044-021-00210-4
Outcome of ductus arteriosus stenting including vertical tubular and convoluted tortuous ducts with emphasis on technical considerations
Abstract
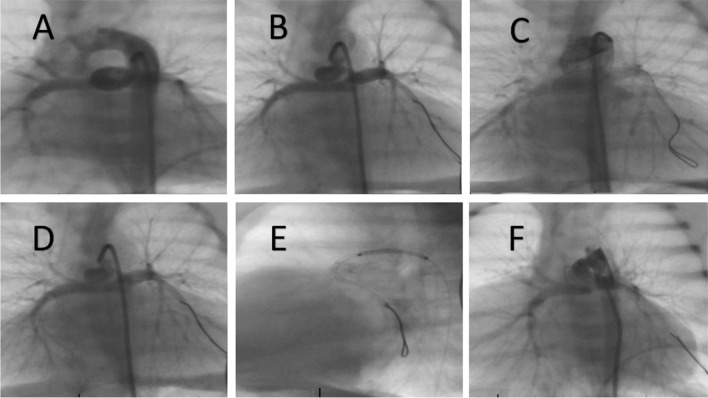
Background: Ductal stenting is the preferred method of securing adequate pulmonary blood flow in patients with duct-dependent pulmonary circulation. The main limitation in most centers is the difficult vertical tubular or convoluted ducts that represent real challenges to interventional pediatric cardiologists. We present our experience in patent ductus arteriosus (PDA) stenting with some technical tips to overcome difficulties, especially in stenting tortuous or long tubular ducts. This study was conducted on all patients with cyanotic congenital heart disease who underwent PDA stenting between January 2011 and December 2018.
Results: We attempted to stent the PDA in 43 patients, with a success rate of 93% (40 patients) and only one procedural mortality. There was also one stent migration that needed to be treated with urgent surgery. Three-fourths of the patients had difficult ductal morphology and origin. One stent was used to cover the PDA in 27 patients (62.8%), two stents were used in 13 (30.2%), and three stents were used in 2 patients (4.6%). In-stent stenosis rate was 12.5% (5 patients) and the development of progressive left pulmonary artery stenosis was seen in two patients (5%). Pulmonary artery growth was adequate in all patients.
Conclusions: PDA stenting is an effective method of palliation for patients with duct-dependent pulmonary circulation. It has low morbidity and mortality rates. Stenting difficult ducts have become more feasible with evolving materials and techniques.
Keywords: Duct-dependent pulmonary; Patent ductus arteriosus; Single ventricle palliation; Stenting.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





References
-
- Glatz AC, Petit CJ, Goldstein BH, Kelleman MS, McCracken CE, McDonnell A, et al. A comparison between patent ductus arteriosus stent and modified Blalock–Taussig shunt as palliation for infants with ductal-dependent pulmonary blood flow: insights from the congenital catheterization research collaborative. Circulation. 2018;137(6):589–601. doi: 10.1161/CIRCULATIONAHA.117.029987. - DOI - PubMed
-
- Bentham JR, Zava NK, Harrison WJ, Shauq A, Kalantre A, Derrick G, et al. Duct stenting versus modified Blalock Taussig shunt in neonates with duct-dependent pulmonary blood flow: associations with clinical outcomes in a multicenter national study. Circulation. 2018;137(6):581–588. doi: 10.1161/CIRCULATIONAHA.117.028972. - DOI - PubMed
LinkOut - more resources
Full Text Sources