

One-Year Committed Exercise Training Reverses Abnormal Left Ventricular Myocardial Stiffness in Patients With Stage B Heart Failure With Preserved Ejection Fraction
- PMID: 34543068
- PMCID: PMC8849598
- DOI: 10.1161/CIRCULATIONAHA.121.054117
One-Year Committed Exercise Training Reverses Abnormal Left Ventricular Myocardial Stiffness in Patients With Stage B Heart Failure With Preserved Ejection Fraction
Abstract
Background: Individuals with left ventricular (LV) hypertrophy and elevated cardiac biomarkers in middle age are at increased risk for the development of heart failure with preserved ejection fraction. Prolonged exercise training reverses the LV stiffening associated with healthy but sedentary aging; however, whether it can also normalize LV myocardial stiffness in patients at high risk for heart failure with preserved ejection fraction is unknown. In a prospective, randomized controlled trial, we hypothesized that 1-year prolonged exercise training would reduce LV myocardial stiffness in patients with LV hypertrophy.
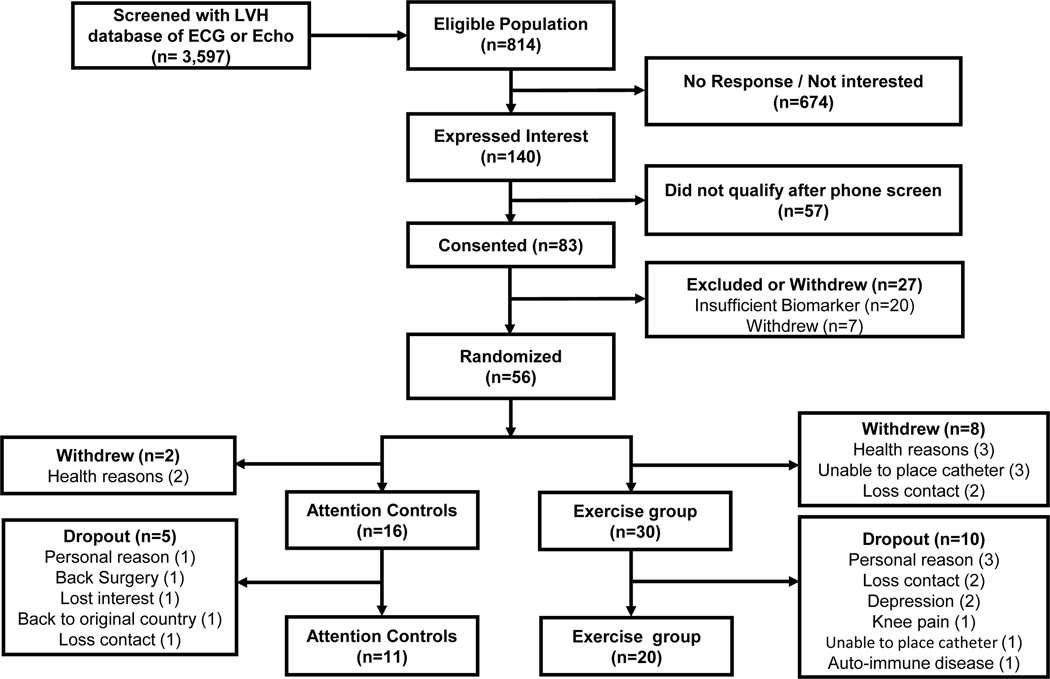
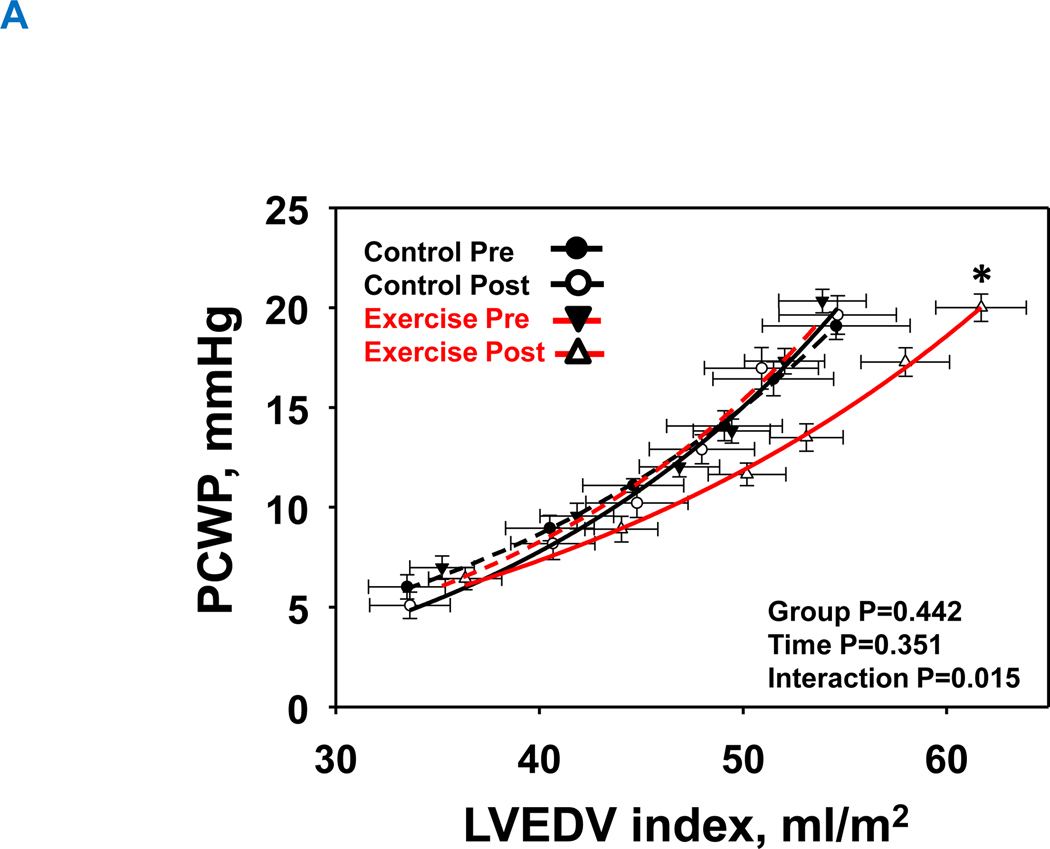
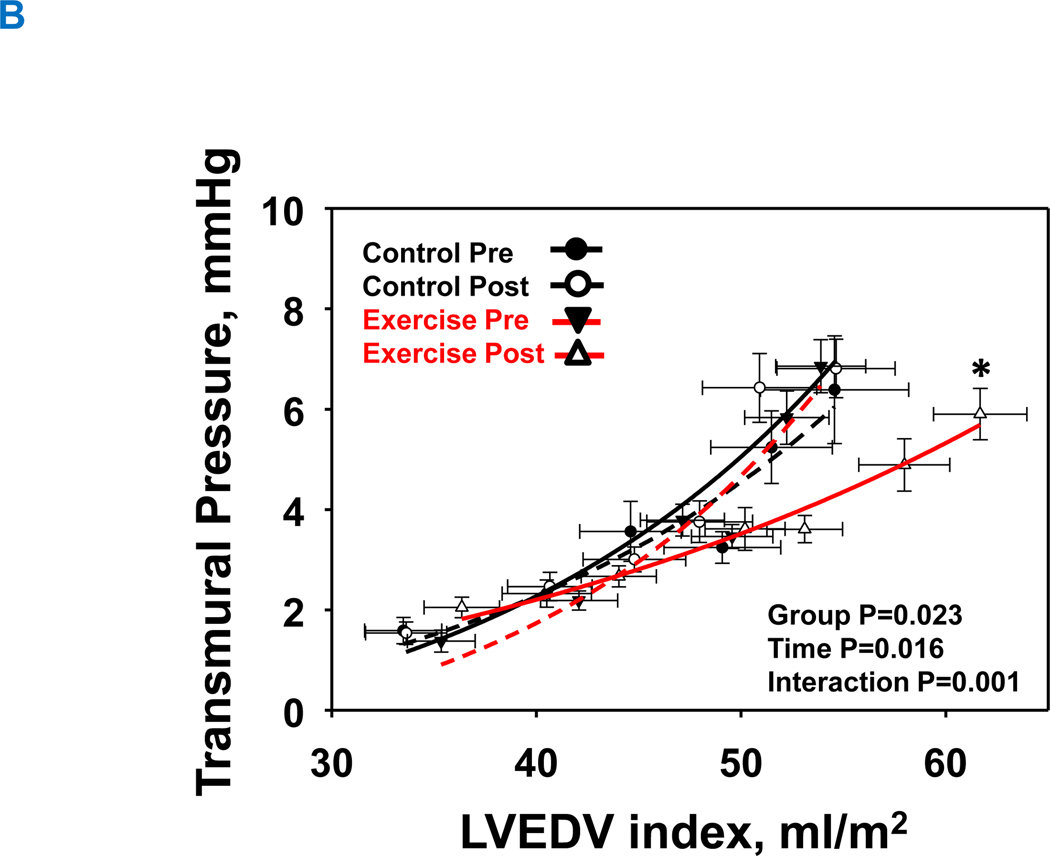
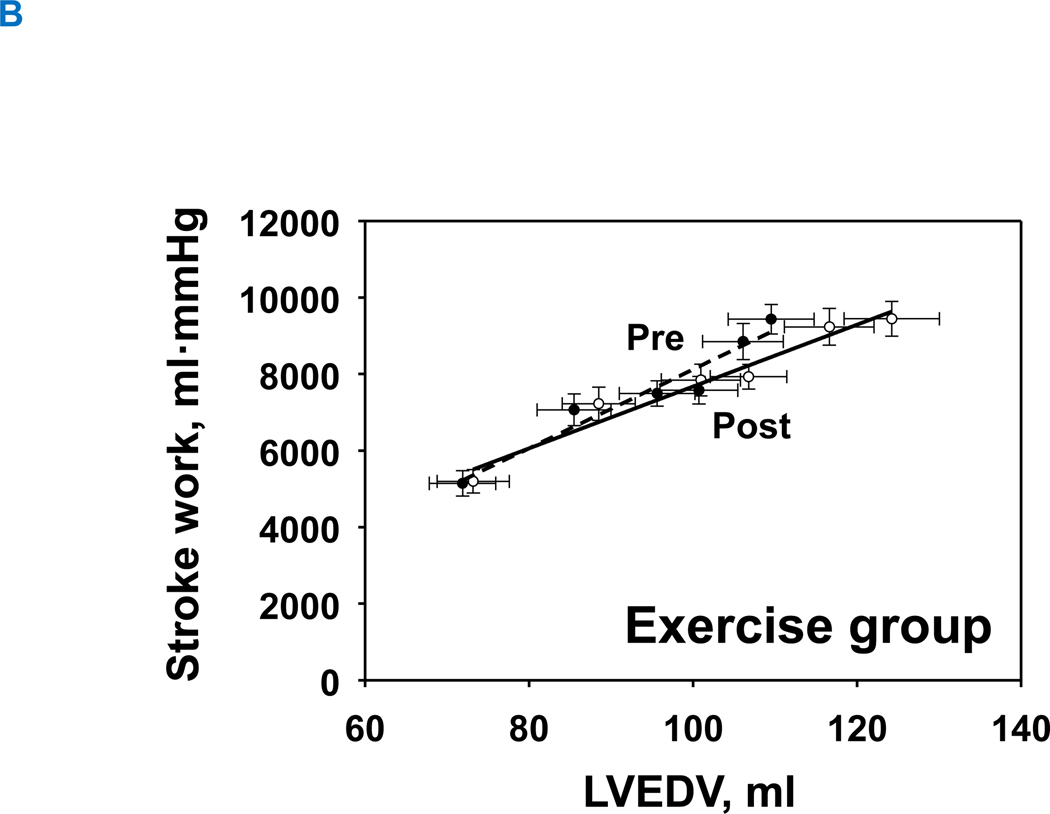
Methods: Forty-six patients with LV hypertrophy (LV septum >11 mm) and elevated cardiac biomarkers (N-terminal pro-B-type natriuretic peptide [>40 pg/mL] or high-sensitivity troponin T [>0.6 pg/mL]) were randomly assigned to either 1 year of high-intensity exercise training (n=30) or attention control (n=16). Right-heart catheterization and 3-dimensional echocardiography were performed while preload was manipulated using both lower body negative pressure and rapid saline infusion to define the LV end-diastolic pressure-volume relationship. A constant representing LV myocardial stiffness was calculated from the following: P=S×[Exp {a (V-V0)}-1], where "P" is transmural pressure (pulmonary capillary wedge pressure - right atrial pressure), "S" is the pressure asymptote of the curve, "V" is the LV end-diastolic volume index, "V0" is equilibrium volume, and "a" is the constant that characterizes LV myocardial stiffness.
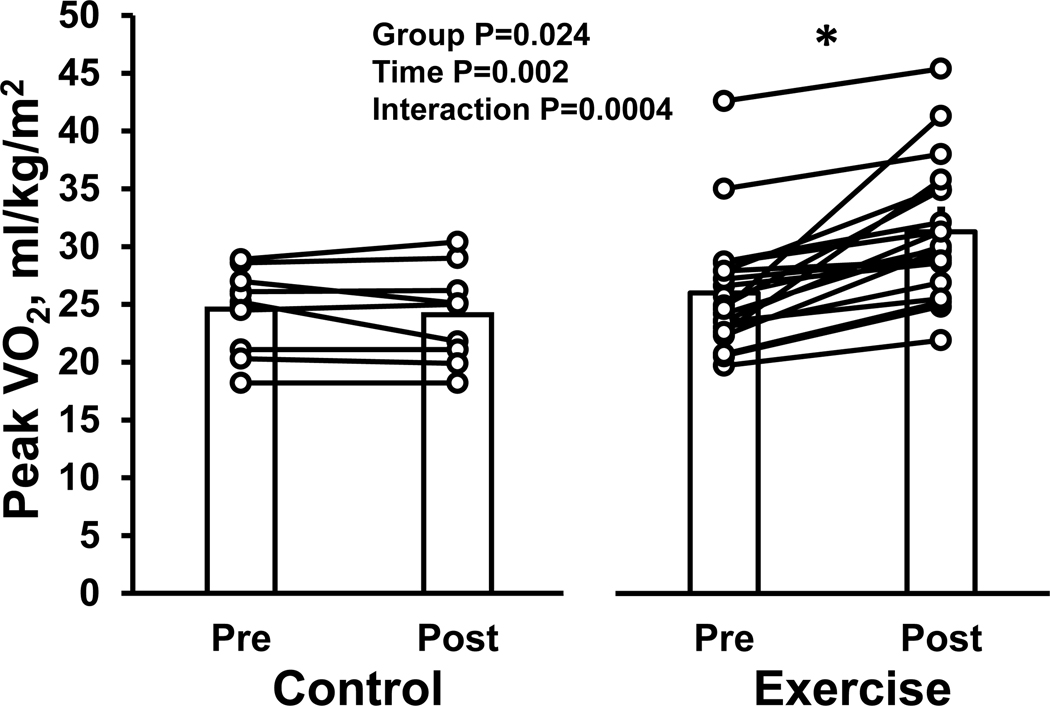
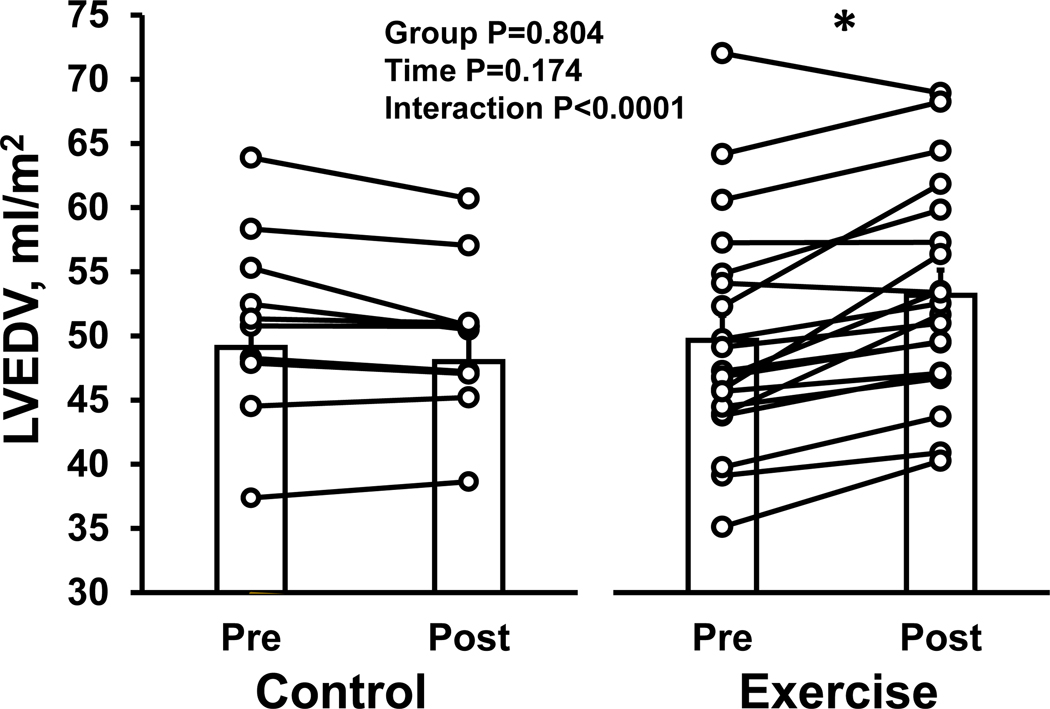
Results: Thirty-one participants (exercise group [n=20]: 54±6 years, 65% male; and controls (n=11): 51±6 years, 55% male) completed the study. One year of exercise training increased max by 21% (baseline 26.0±5.3 to 1 year later 31.3±5.8 mL·min-1·kg-1, P<0.0001, interaction P=0.0004), whereas there was no significant change in max in controls (baseline 24.6±3.4 to 1 year later 24.2±4.1 mL·min-1·kg-1, P=0.986). LV myocardial stiffness was reduced (right and downward shift in the end-diastolic pressure-volume relationship; LV myocardial stiffness: baseline 0.062±0.020 to 1 year later 0.031±0.009), whereas there was no significant change in controls (baseline 0.061±0.033 to 1 year later 0.066±0.031, interaction P=0.001).
Conclusions: In patients with LV hypertrophy and elevated cardiac biomarkers (stage B heart failure with preserved ejection fraction), 1 year of exercise training reduced LV myocardial stiffness. Thus, exercise training may provide protection against the future risk of heart failure with preserved ejection fraction in such patients. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT03476785.
Keywords: blood volume; heart failure; hypertrophy, left ventricular; vascular stiffness.
Figures
Comment in
-
Letter by Lucas and Taegtmeyer Regarding Article, "One-Year Committed Exercise Training Reverses Abnormal Left Ventricular Myocardial Stiffness in Patients With Stage B Heart Failure With Preserved Ejection Fraction".Circulation. 2022 Mar;145(9):e642-e643. doi: 10.1161/CIRCULATIONAHA.121.058145. Epub 2022 Feb 28. Circulation. 2022. PMID: 35226553 Free PMC article. No abstract available.
-
Response by Hieda and Levine to Letter Regarding Article, "One-Year Committed Exercise Training Reverses Abnormal Left Ventricular Myocardial Stiffness in Patients With Stage B Heart Failure With Preserved Ejection Fraction".Circulation. 2022 Mar;145(9):e644. doi: 10.1161/CIRCULATIONAHA.122.058733. Epub 2022 Feb 28. Circulation. 2022. PMID: 35226555 No abstract available.
References
-
- Zile MR, Baicu CF and Gaasch WH. Diastolic heart failure--abnormalities in active relaxation and passive stiffness of the left ventricle. The New England journal of medicine. 2004;350:1953–1959. - PubMed
-
- Kawaguchi M, Hay I, Fetics B and Kass DA. Combined ventricular systolic and arterial stiffening in patients with heart failure and preserved ejection fraction: implications for systolic and diastolic reserve limitations. Circulation. 2003;107:714–720. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
