

Prevalence of Subclinical Coronary Artery Atherosclerosis in the General Population
- PMID: 34543072
- PMCID: PMC8448414
- DOI: 10.1161/CIRCULATIONAHA.121.055340
Prevalence of Subclinical Coronary Artery Atherosclerosis in the General Population
Abstract
Background: Early detection of coronary atherosclerosis using coronary computed tomography angiography (CCTA), in addition to coronary artery calcification (CAC) scoring, may help inform prevention strategies. We used CCTA to determine the prevalence, severity, and characteristics of coronary atherosclerosis and its association with CAC scores in a general population.
Methods: We recruited 30 154 randomly invited individuals age 50 to 64 years to SCAPIS (the Swedish Cardiopulmonary Bioimage Study). The study includes individuals without known coronary heart disease (ie, no previous myocardial infarctions or cardiac procedures) and with high-quality results from CCTA and CAC imaging performed using dedicated dual-source CT scanners. Noncontrast images were scored for CAC. CCTA images were visually read and scored for coronary atherosclerosis per segment (defined as no atherosclerosis, 1% to 49% stenosis, or ≥50% stenosis). External validity of prevalence estimates was evaluated using inverse probability for participation weighting and Swedish register data.
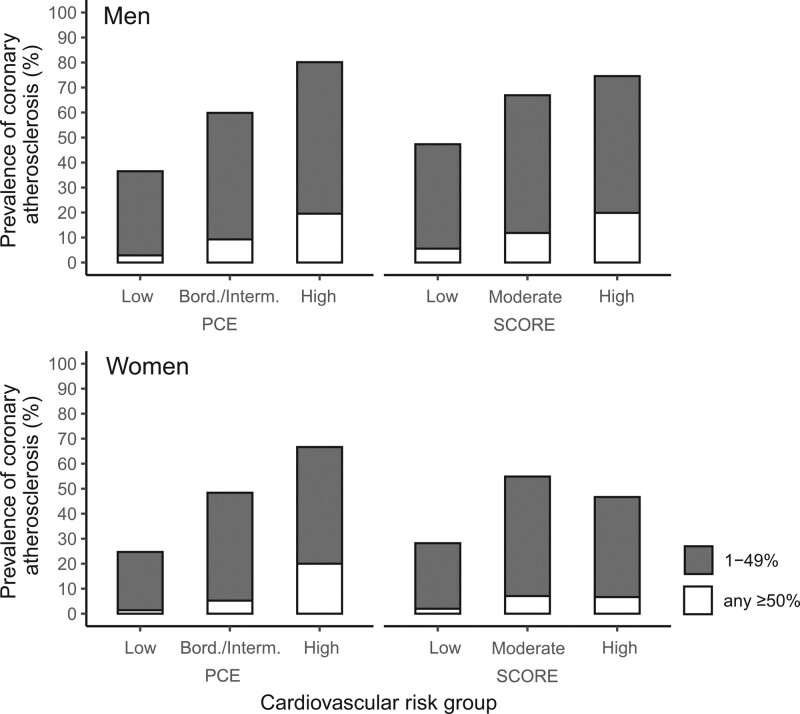
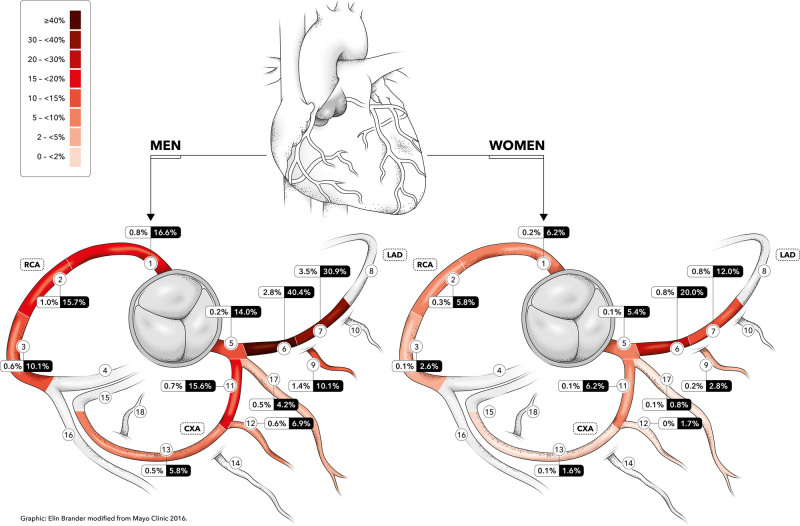
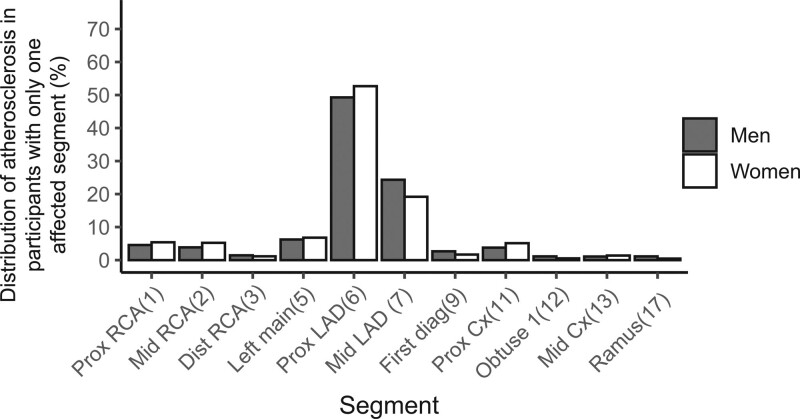
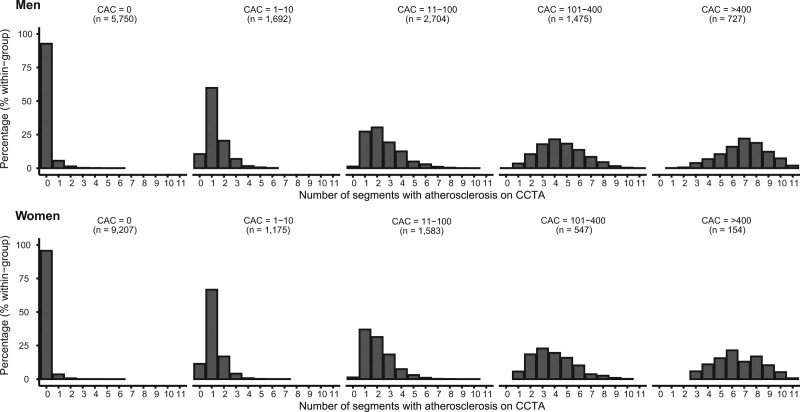
Results: In total, 25 182 individuals without known coronary heart disease were included (50.6% women). Any CCTA-detected atherosclerosis was found in 42.1%; any significant stenosis (≥50%) in 5.2%; left main, proximal left anterior descending artery, or 3-vessel disease in 1.9%; and any noncalcified plaques in 8.3% of this population. Onset of atherosclerosis was delayed on average by 10 years in women. Atherosclerosis was more prevalent in older individuals and predominantly found in the proximal left anterior descending artery. Prevalence of CCTA-detected atherosclerosis increased with increasing CAC scores. Among those with a CAC score >400, all had atherosclerosis and 45.7% had significant stenosis. In those with 0 CAC, 5.5% had atherosclerosis and 0.4% had significant stenosis. In participants with 0 CAC and intermediate 10-year risk of atherosclerotic cardiovascular disease according to the pooled cohort equation, 9.2% had CCTA-verified atherosclerosis. Prevalence estimates had excellent external validity and changed marginally when adjusted to the age-matched Swedish background population.
Conclusions: Using CCTA in a large, random sample of the general population without established disease, we showed that silent coronary atherosclerosis is common in this population. High CAC scores convey a significant probability of substantial stenosis, and 0 CAC does not exclude atherosclerosis, particularly in those at higher baseline risk.
Keywords: coronary angiography; coronary artery disease; epidemiology; plaque, atherosclerotic; primary prevention; tomography.
Figures
Comment in
-
Population Screening With Coronary Computed Tomography Angiography and the Prevention of Coronary Events.Circulation. 2021 Sep 21;144(12):930-933. doi: 10.1161/CIRCULATIONAHA.121.055784. Epub 2021 Sep 20. Circulation. 2021. PMID: 34543070 No abstract available.
References
-
- Björck L, Rosengren A, Bennett K, Lappas G, Capewell S. Modelling the decreasing coronary heart disease mortality in Sweden between 1986 and 2002. Eur Heart J. 2009; 30:1046–1056. doi:10.1093/eurheartj/ehn554 - PubMed
-
- The Swedish National Board of Health and Welfare. Health and Medical Care: Statistics on Myocardial Infarctions 2019. The Swedish National Board of Health and Welfare. 20201–5. https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelk...
-
- Emberson J, Whincup P, Morris R, Walker M, Ebrahim S. Evaluating the impact of population and high-risk strategies for the primary prevention of cardiovascular disease. Eur Heart J. 2004; 25:484–491. doi: 10.1016/j.ehj.2003.11.012 - PubMed
-
- Burke AP, Farb A, Malcom GT, Liang YH, Smialek J, Virmani R. Coronary risk factors and plaque morphology in men with coronary disease who died suddenly. N Engl J Med. 1997; 336:1276–1282. doi: 10.1056/NEJM199705013361802 - PubMed
-
- Stone GW, Maehara A, Lansky AJ, de Bruyne B, Cristea E, Mintz GS, Mehran R, McPherson J, Farhat N, Marso SP, et al. PROSPECT Investigators. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011; 364:226–235. doi: 10.1056/NEJMoa1002358 - PubMed
