

Surveillance for peri-elimination trachoma recrudescence: Exploratory studies in Ghana
- PMID: 34543293
- PMCID: PMC8519445
- DOI: 10.1371/journal.pntd.0009744
Surveillance for peri-elimination trachoma recrudescence: Exploratory studies in Ghana
Abstract
Introduction: To date, eleven countries have been validated as having eliminated trachoma as a public health problem, including Ghana in 2018. Surveillance for recrudescence is needed both pre- and post-validation but evidence-based guidance on appropriate strategies is lacking. We explored two potential surveillance strategies in Ghana.
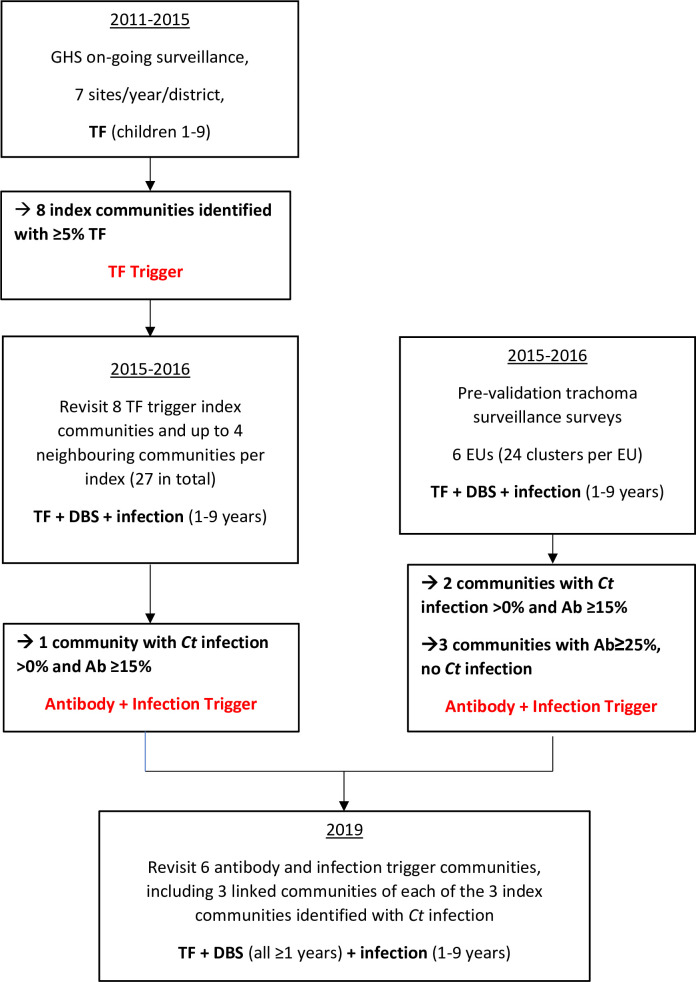
Methodology/principal findings: Amongst randomly-selected communities enrolled in pre-validation on-going surveillance between 2011 and 2015, eight were identified as having had trachomatous-inflammation follicular (TF) prevalence ≥5% in children aged 1-9 years between 2012 and 2014. These eight were re-visited in 2015 and 2016 and neighbouring communities were also added ("TF trigger" investigations). Resident children aged 1-9 years were then examined for trachoma and had a conjunctival swab to test for Chlamydia trachomatis (Ct) and a dried blood spot (DBS) taken to test for anti-Pgp3 antibodies. These investigations identified at least one community with evidence of probable recent Ct ocular transmission. However, the approach likely lacks sufficient spatio-temporal power to be reliable. A post-validation surveillance strategy was also evaluated, this reviewed the ocular Ct infection and anti-Pgp3 seroprevalence data from the TF trigger investigations and from the pre-validation surveillance surveys in 2015 and 2016. Three communities identified as having ocular Ct infection >0% and anti-Pgp3 seroprevalence ≥15.0% were identified, and along with three linked communities, were followed-up as part of the surveillance strategy. An additional three communities with a seroprevalence ≥25.0% but no Ct infection were also followed up ("antibody and infection trigger" investigations). DBS were taken from all residents aged ≥1 year and ocular swabs from all children aged 1-9 years. There was evidence of transmission in the group of communities visited in one district (Zabzugu-Tatale). There was no or little evidence of continued transmission in other districts, suggesting previous infection identified was transient or potentially not true ocular Ct infection.
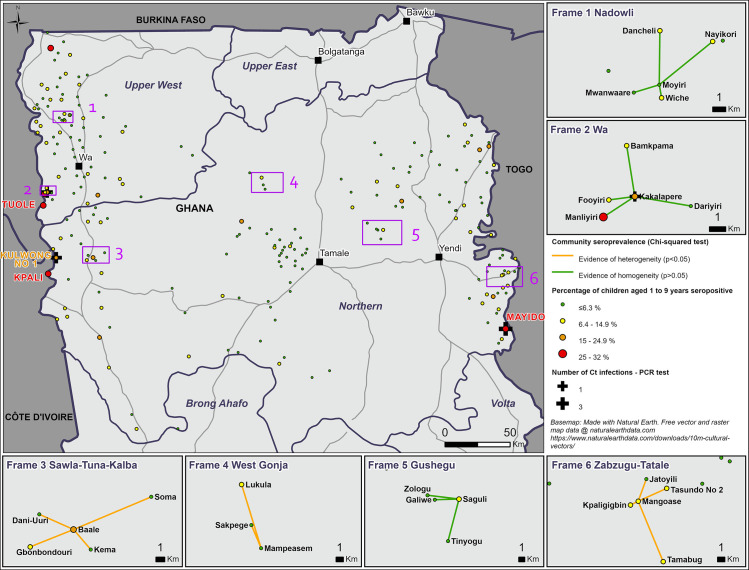
Conclusions/significance: There is evidence of heterogeneity in Ct transmission dynamics in northern Ghana, even 10 years after wide-scale MDA has stopped. There is added value in monitoring Ct infection and anti-Ct antibodies, using these indicators to interrogate past or present surveillance strategies. This can result in a deeper understanding of transmission dynamics and inform new post-validation surveillance strategies. Opportunities should be explored for integrating PCR and serological-based markers into surveys conducted in trachoma elimination settings.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Assembly. Global elimination of blinding trachoma. 51st World Health Assembly, Geneva, 16 May 1998, Resolution WHA51.11. Geneva: World Health Organization; 1998.
-
- World Health Organization. Validation of elimination of trachoma as a public health problem (WHO/HTM/NTD/2016.8). Geneva: World Health Organization; 2016.
-
- Senyonjo LG, Debrah O, Martin DL, Asante-Poku A, Migchelsen SJ, Gwyn S, et al.. Serological and PCR-based markers of ocular Chlamydia trachomatis transmission in northern Ghana after elimination of trachoma as a public health problem. PLoS Negl Trop Dis. 2018;12(12):e0007027. doi: 10.1371/journal.pntd.0007027 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
