

Nasopharyngeal Codetection of Haemophilus influenzae and Streptococcus pneumoniae Shapes Respiratory Syncytial Virus Disease Outcomes in Children
- PMID: 34543409
- PMCID: PMC8889286
- DOI: 10.1093/infdis/jiab481
Nasopharyngeal Codetection of Haemophilus influenzae and Streptococcus pneumoniae Shapes Respiratory Syncytial Virus Disease Outcomes in Children
Abstract
Background: The role of nasopharyngeal bacteria in respiratory syncytial virus (RSV) disease has been underestimated. We measured the frequency and burden of respiratory bacteria in the upper respiratory tract of infants with RSV infection over 7 respiratory seasons, and their impact on clinical outcomes.
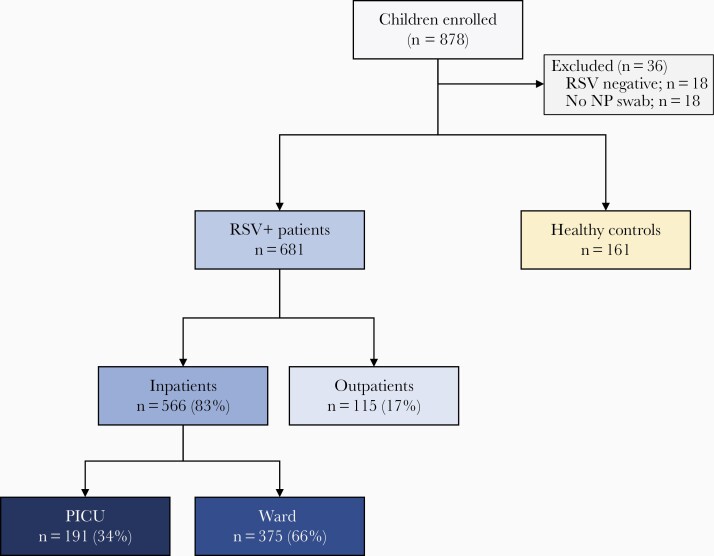
Methods: Children <2 years old with mild (outpatients, n=115) or severe (inpatients, n=566) RSV infection, and matched healthy controls (n=161) were enrolled. Nasopharyngeal samples were obtained for RSV, Streptococcus pneumoniae, Staphylococcus aureus, Moraxella catarrhalis, and Haemophilus influenzae detection and quantitation by PCR. Multivariable models were constructed to identify variables predictive of severe disease.
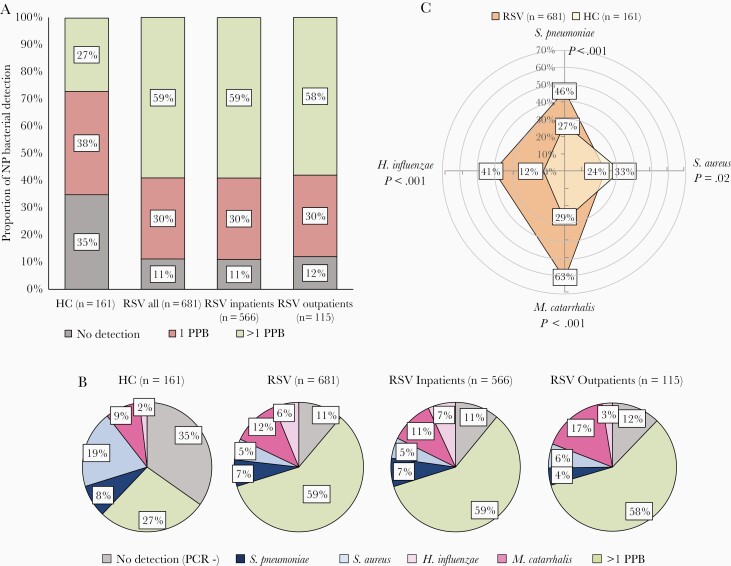
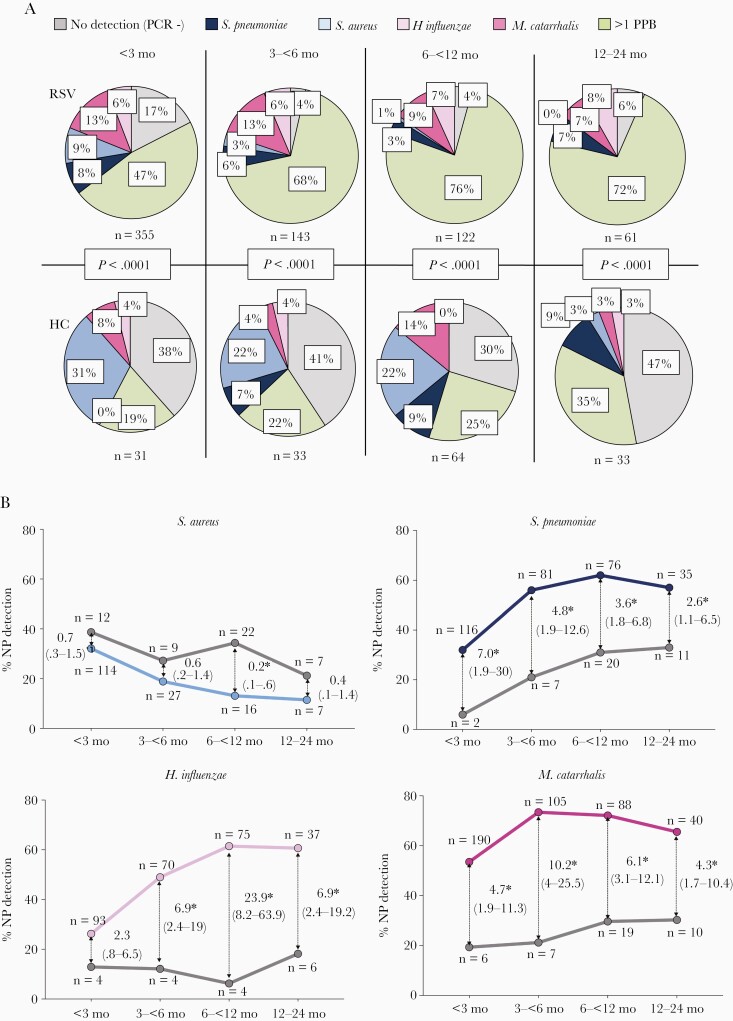
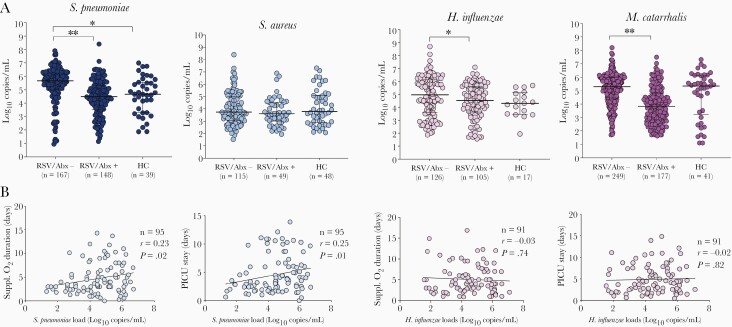
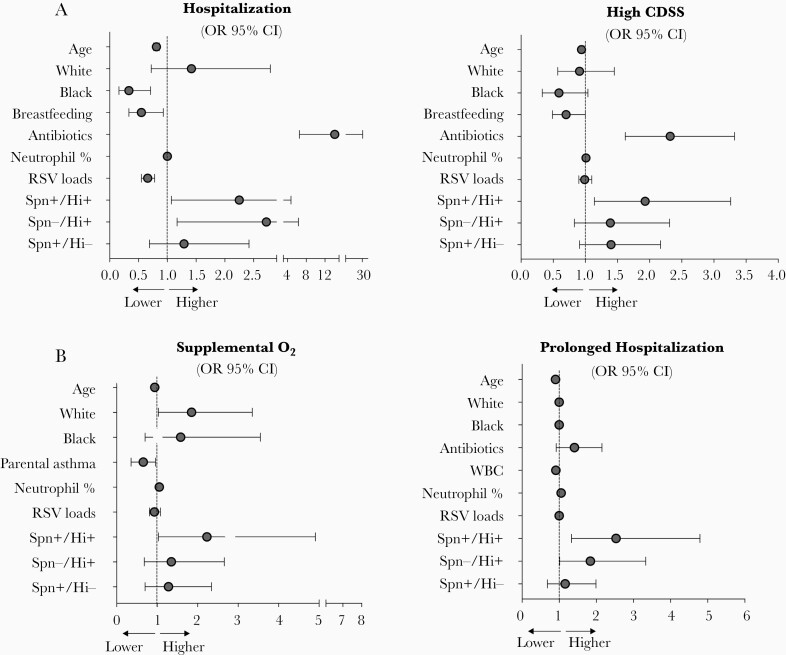
Results: S. pneumoniae, H. influenzae, and M. catarrhalis, but not S. aureus, were detected more frequently in RSV-infected children (84%) than healthy controls (46%; P<.001). Detection of S. pneumoniae and/or H. influenzae was associated with fever, more frequent antibiotic treatment, worse radiologic findings, and higher neutrophil counts (P<.01). In adjusted analyses, S. pneumoniae/H. influenzae codetection was independentlyassociated with greater odds of hospitalization, higher disease severity scores, need for supplemental oxygen, and longer hospitalization.
Conclusions: Nasopharyngeal codetection of S. pneumoniae and H. influenzae in infants with RSV infection is associated with increased disease severity.
Keywords: RSV; bacterial PCR; disease severity; infants; nasopharyngeal bacterial colonization.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
