

What Will It Take to End HIV in the United States? : A Comprehensive, Local-Level Modeling Study
- PMID: 34543589
- PMCID: PMC8595759
- DOI: 10.7326/M21-1501
What Will It Take to End HIV in the United States? : A Comprehensive, Local-Level Modeling Study
Abstract
Background: The Ending the HIV Epidemic (EHE) initiative aims to reduce incident HIV infections by 90% over a span of 10 years. The intensity of interventions needed to achieve this for local epidemics is unclear.
Objective: To estimate the effect of HIV interventions at the city level.
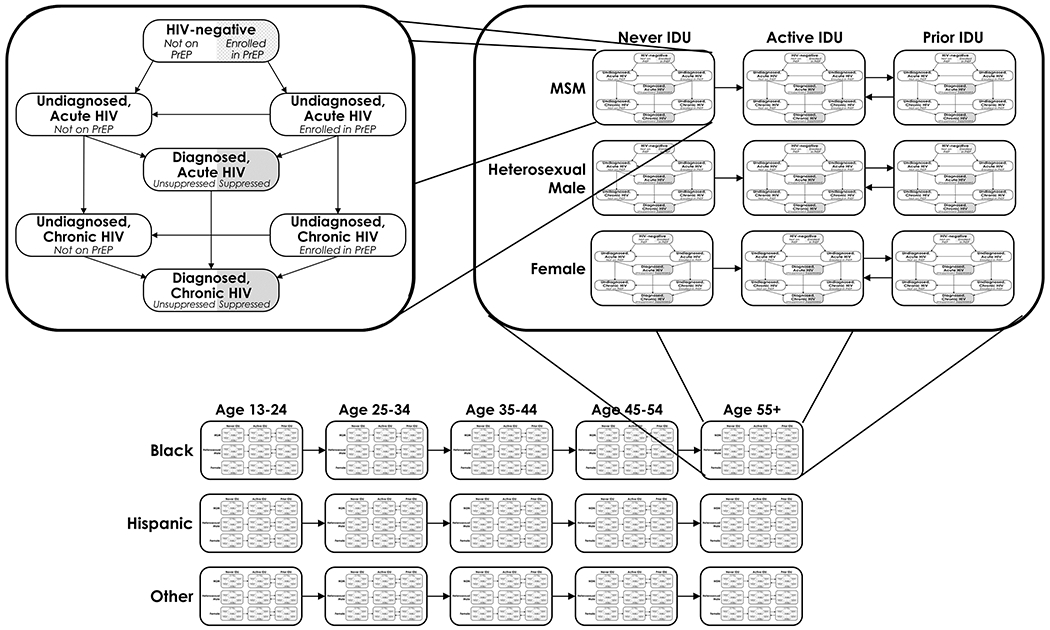
Design: A compartmental model of city-level HIV transmission stratified by age, race, sex, and HIV risk factor was developed and calibrated.
Setting: 32 priority metropolitan statistical areas (MSAs).
Patients: Simulated populations in each MSA.
Intervention: Combinations of HIV testing and preexposure prophylaxis (PrEP) coverage among those at risk for HIV, plus viral suppression in persons with diagnosed HIV infection.
Measurements: The primary outcome was the projected reduction in incident cases from 2020 to 2030.
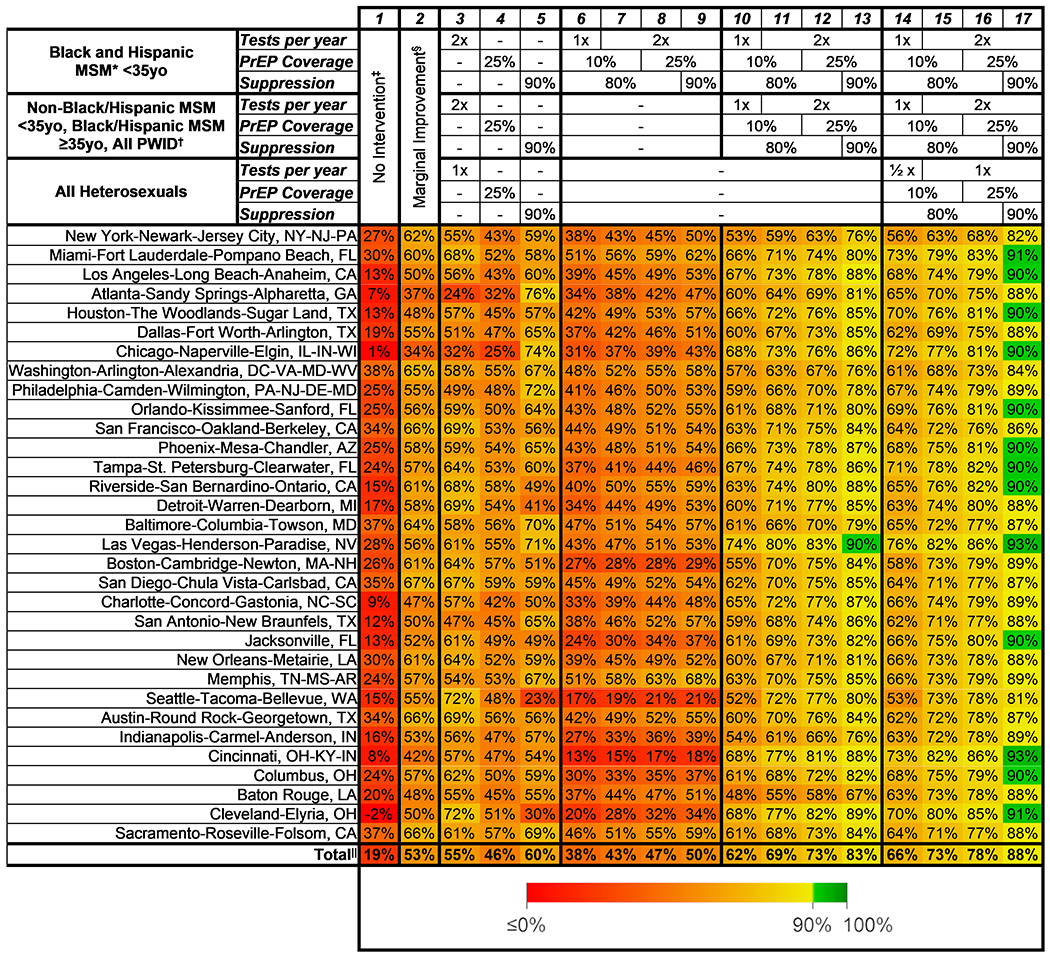
Results: Absent intervention, HIV incidence was projected to decrease by 19% across all 32 MSAs. Modest increases in testing (1.25-fold per year), PrEP coverage (5 percentage points), and viral suppression (10 percentage points) across the population could achieve reductions of 34% to 67% by 2030. Twenty-five percent PrEP coverage, testing twice a year on average, and 90% viral suppression among young Black and Hispanic men who have sex with men (MSM) achieved similar reductions (13% to 68%). Including all MSM and persons who inject drugs could reduce incidence by 48% to 90%. Thirteen of 32 MSAs could achieve greater than 90% reductions in HIV incidence with large-scale interventions that include heterosexuals. A web application with location-specific results is publicly available (www.jheem.org).
Limitation: The COVID-19 pandemic was not represented.
Conclusion: Large reductions in HIV incidence are achievable with substantial investment, but the EHE goals will be difficult to achieve in most locations. An interactive model that can help policymakers maximize the effect in their local environments is presented.
Primary funding source: National Institutes of Health.
Figures


Comment in
-
Ending HIV in the United States Will Require a Substantial Financial Commitment.Ann Intern Med. 2021 Nov;174(11):1620-1621. doi: 10.7326/M21-3607. Epub 2021 Sep 21. Ann Intern Med. 2021. PMID: 34543585 No abstract available.
References
-
- Centers for Disease Control and Prevention. Diagnoses of HIV infection in the United States and dependent areas, 2018 (updated). HIV Surveillance Report. 2020;31:1–119. Accessed at www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-re... on 5/1/2021.
-
- Panagiotoglou D, Olding M, Enns B, et al. ; Localized HIV Modeling Study Group. Building the case for localized approaches to HIV: structural conditions and health system capacity to address the HIV/AIDS epidemic in six US cities. AIDS Behav. 2018;22:3071–3082. doi: 10.1007/s10461-018-2166-6 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous