

Kidney Disease, Hypertension Treatment, and Cerebral Perfusion and Structure
- PMID: 34543687
- PMCID: PMC8926938
- DOI: 10.1053/j.ajkd.2021.07.024
Kidney Disease, Hypertension Treatment, and Cerebral Perfusion and Structure
Abstract
Rationale & objective: The safety of intensive blood pressure (BP) targets is controversial for persons with chronic kidney disease (CKD). We studied the effects of hypertension treatment on cerebral perfusion and structure in individuals with and without CKD.
Study design: Neuroimaging substudy of a randomized trial.
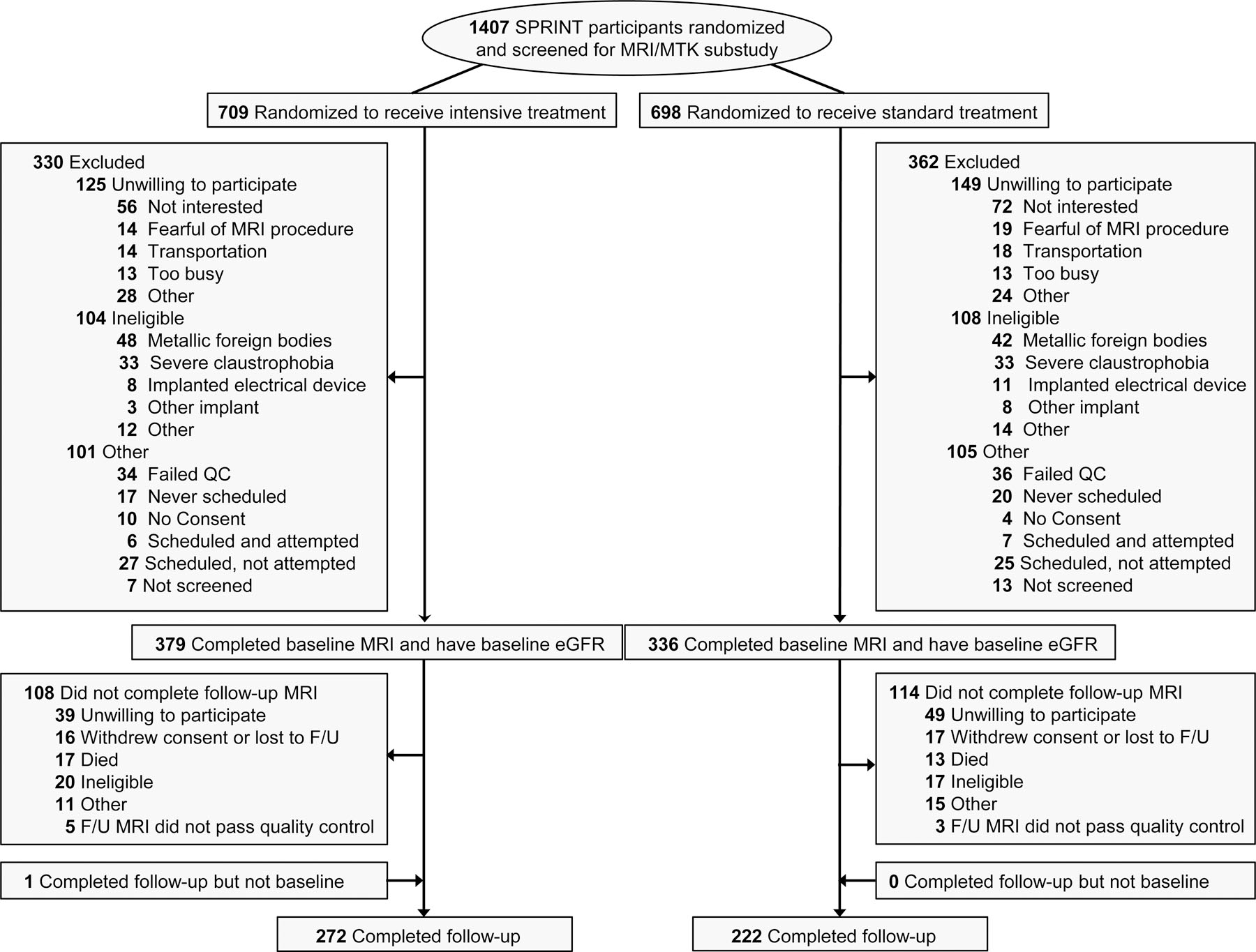
Setting & participants: A subset of participants in the Systolic Blood Pressure Intervention Trial (SPRINT) who underwent brain magnetic resonance imaging studies. Presence of baseline CKD was assessed by estimated glomerular filtration rate (eGFR) and urinary albumin-creatinine ratio (UACR).
Intervention: Participants were randomly assigned to intensive (systolic BP <120 mm Hg) versus standard (systolic BP <140 mm Hg) BP lowering.
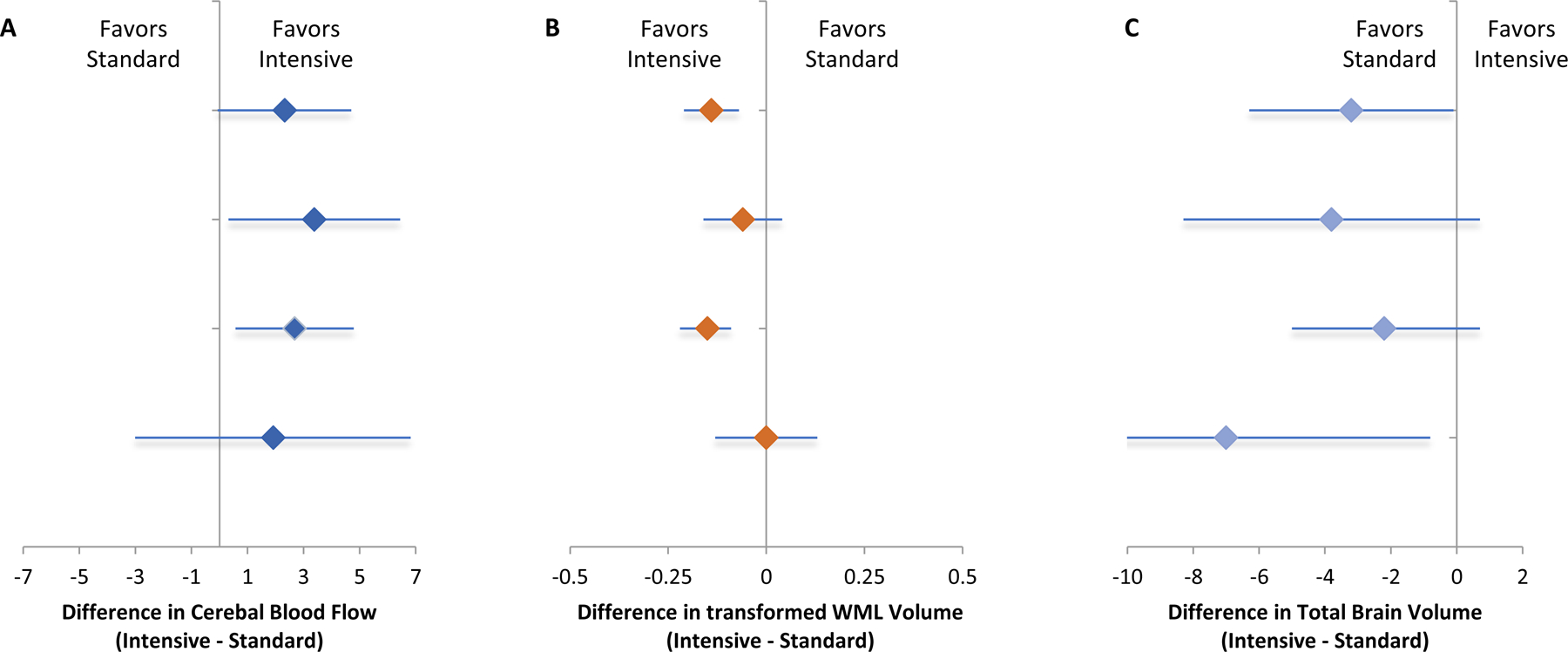
Outcomes: The magnetic resonance imaging outcome measures were the 4-year change in global cerebral blood flow (CBF), white matter lesion (WML) volume, and total brain volume (TBV).
Results: A total of 716 randomized participants with a mean age of 68 years were enrolled; follow-up imaging occurred after a median 3.9 years. Among participants with eGFR <60 mL/min/1.73 m2 (n = 234), the effects of intensive versus standard BP treatment on change in global CBF, WMLs, and TBV were 3.38 (95% CI, 0.32 to 6.44) mL/100 g/min, -0.06 (95% CI, -0.16 to 0.04) cm3 (inverse hyperbolic sine-transformed), and -3.8 (95% CI, -8.3 to 0.7) cm3, respectively. Among participants with UACR >30 mg/g (n = 151), the effects of intensive versus standard BP treatment on change in global CBF, WMLs, and TBV were 1.91 (95% CI, -3.01 to 6.82) mL/100 g/min, 0.003 (95% CI, -0.13 to 0.13) cm3 (inverse hyperbolic sine-transformed), and -7.0 (95% CI, -13.3 to -0.3) cm3, respectively. The overall treatment effects on CBF and TBV were not modified by baseline eGFR or UACR; however, the effect on WMLs was attenuated in participants with albuminuria (P = 0.04 for interaction).
Limitations: Measurement variability due to multisite design.
Conclusions: Among adults with hypertension who have primarily early kidney disease, intensive versus standard BP treatment did not appear to have a detrimental effect on brain perfusion or structure. The findings support the safety of intensive BP treatment targets on brain health in persons with early kidney disease.
Funding: SPRINT was funded by the National Institutes of Health (including the National Heart, Lung, and Blood Institute; the National Institute of Diabetes and Digestive and Kidney Diseases; the National Institute on Aging; and the National Institute of Neurological Disorders and Stroke), and this substudy was funded by the National Institutes of Diabetes and Digestive and Kidney Diseases.
Trial registration: SPRINT was registered at ClinicalTrials.gov with study number NCT01206062.
Keywords: Hypertension; albuminuria; blood pressure (BP); cerebral perfusion; chronic kidney disease (CKD); intensive BP control; magnetic resonance imaging (MRI); neuroimaging; white matter injury; white matter lesions.
Published by Elsevier Inc.
Conflict of interest statement
Figures
References
-
- Seliger SL, Siscovick DS, Stehman-Breen CO, et al. Moderate Renal Impairment and Risk of Dementia among Older Adults: The Cardiovascular Health Cognition Study. J Am Soc Nephrol 2004;15(7):1904–1911. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UL1 TR000433/TR/NCATS NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- UL1 TR000064/TR/NCATS NIH HHS/United States
- UL1 TR000075/TR/NCATS NIH HHS/United States
- UL1 TR000093/TR/NCATS NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- P30 AG072947/AG/NIA NIH HHS/United States
- R01 AG055606/AG/NIA NIH HHS/United States
- HHSN268200900048C/HL/NHLBI NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- R03 AG063213/AG/NIA NIH HHS/United States
- HHSN268200900040C/HL/NHLBI NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- HHSN268200900046C/HL/NHLBI NIH HHS/United States
- U24 DK060990/DK/NIDDK NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- UL1 TR001064/TR/NCATS NIH HHS/United States
- UL1 RR025752/RR/NCRR NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
- HHSN268200900049C/HL/NHLBI NIH HHS/United States
- HHSN268200900047C/HL/NHLBI NIH HHS/United States
- R01 DK092241/DK/NIDDK NIH HHS/United States
- UL1 TR000050/TR/NCATS NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 TR000073/TR/NCATS NIH HHS/United States
- UL1 RR025755/RR/NCRR NIH HHS/United States
- S10 OD023495/OD/NIH HHS/United States
- UL1 TR000002/TR/NCATS NIH HHS/United States
- UL1 TR000105/TR/NCATS NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
- UL1 TR003142/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
