Evaluation of atrial fibrosis in atrial fibrillation patients with three different methods
- PMID: 34544218
- PMCID: PMC10734846
- DOI: 10.3906/sag-2103-194
Evaluation of atrial fibrosis in atrial fibrillation patients with three different methods
Abstract
Background: The presence of atrial fibrosis has already been known as a risk factor for atrial fibrillation (AF) development. We aimed to evaluate atrial fibrosis with previously defined three different methods, which were cardiac magnetic resonance imaging (C-MRI), echocardiographic strain imaging, and biomarkers and show the relationship between these methods in patients with AF scheduled for cryoballoon ablation.
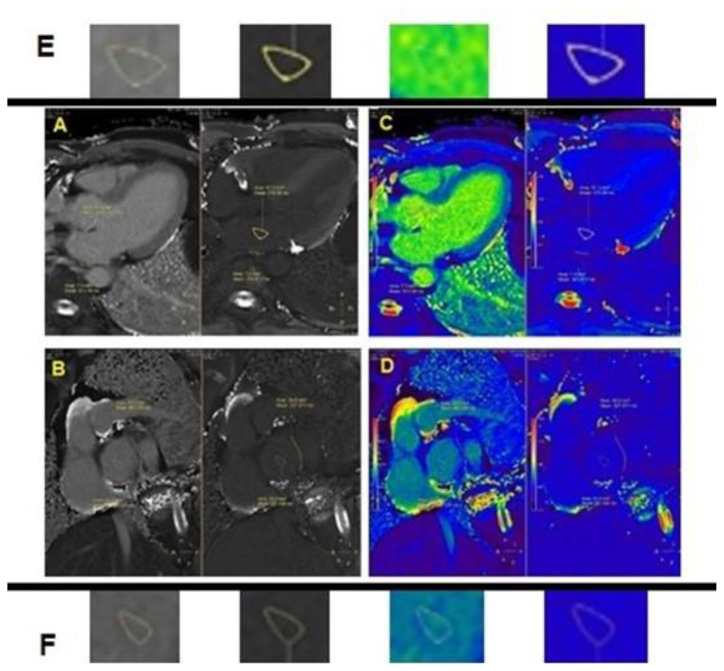
Methods: A total of 30 patients were enrolled. Atrial T1 relaxation durations were measured using C-MRI before the procedure of atrial fibrillation catheter ablation. Fibroblast growth factor-21 (FGF-21) and fibroblast growth factor-23 (FGF-23) levels were measured at serum derived from the femoral artery (Peripheral FGF 21 and 23) and left atrium blood samples (Central FGF 21 and 23) before catheter ablation. Preprocedural transthoracic echocardiography was performed. The median follow-up duration for atrial tachyarrhythmia (ATa) recurrence was 13 (12-18 months) months.
Results: The mean ages of the study group were 55.23 ± 12.37 years, and there were 17 (56.7%) female patients in study population. There were negative correlations between post contrast T1 relaxation durations of both posterior and posterosuperior atrium, and central FGF-23 (r: - 0.561; p = 0.003; r:-0.624; p = 0.001; Posterior T1 vs. central FGF-23 levels and Posterosuperior T1 vs central FGF-23 levels, respectively). The positive correlations were observed between postcontrast posterior T1 relaxation durations and left ventricle ejection fraction (r:0.671; p = 0.001); left atrial emptying fraction (r:0.482; p = 0.013); peak atrial longitudinal strain (r:0.605; p = 0.001), and peak atrial contraction strain (r:0.604; p = 0.001). Also negative correlation was observed between postcontrast posterior T1 relaxation durations, and left atrial volume index (r: - 0.467; p = 0.016).
Keywords: Atrial fibrillation; FGF-21; FGF-23; atrial fibrosis; atrial strain imaging; cardiac MRI T1 relaxation duration.
Figures



Similar articles
-
Magnetic resonance post-contrast T1 mapping in the human atrium: validation and impact on clinical outcome after catheter ablation for atrial fibrillation.Heart Rhythm. 2014 Sep;11(9):1551-9. doi: 10.1016/j.hrthm.2014.06.012. Epub 2014 Jun 12. Heart Rhythm. 2014. PMID: 24931636
-
Clinical utility of cardiac magnetic resonance imaging to assess the left atrium before catheter ablation for atrial fibrillation - A systematic review and meta-analysis.Int J Cardiol. 2021 Sep 15;339:192-202. doi: 10.1016/j.ijcard.2021.07.030. Epub 2021 Jul 23. Int J Cardiol. 2021. PMID: 34303756
-
Diffuse ventricular fibrosis measured by T₁ mapping on cardiac MRI predicts success of catheter ablation for atrial fibrillation.Circ Arrhythm Electrophysiol. 2014 Oct;7(5):834-40. doi: 10.1161/CIRCEP.114.001479. Epub 2014 Aug 20. Circ Arrhythm Electrophysiol. 2014. PMID: 25141860
-
Intra-cardiac and peripheral levels of biochemical markers of fibrosis in patients undergoing catheter ablation for atrial fibrillation.Europace. 2017 Dec 1;19(12):1944-1950. doi: 10.1093/europace/euw315. Europace. 2017. PMID: 28339804
-
The association of baseline left atrial structure and function measured with cardiac magnetic resonance and pulmonary vein isolation outcome in patients with drug-refractory atrial fibrillation.Heart Rhythm. 2016 May;13(5):1037-1044. doi: 10.1016/j.hrthm.2016.01.016. Epub 2016 Jan 14. Heart Rhythm. 2016. PMID: 26775143
Cited by
-
Left atrial strain predicts paroxysmal atrial fibrillation recurrence after catheter ablation: a 1-year study using three-dimensional speckle-tracking echocardiography.BMC Cardiovasc Disord. 2025 Feb 4;25(1):78. doi: 10.1186/s12872-024-04447-0. BMC Cardiovasc Disord. 2025. PMID: 39905319 Free PMC article.
-
Echocardiographic assessment of atrial, ventricular, and valvular function in patients with atrial fibrillation-an expert proposal by the german working group of cardiovascular ultrasound.Clin Res Cardiol. 2025 Jan;114(1):4-24. doi: 10.1007/s00392-024-02491-6. Epub 2024 Aug 26. Clin Res Cardiol. 2025. PMID: 39186180 Free PMC article. Review.
-
Predictive Value of Serum microRNA-29b-3p in Recurrence of Atrial Fibrillation After Radiofrequency Catheter Ablation.Clin Interv Aging. 2024 May 3;19:715-725. doi: 10.2147/CIA.S450292. eCollection 2024. Clin Interv Aging. 2024. PMID: 38716143 Free PMC article.
-
Biomarkers of Atrial Fibrillation Recurrence in Patients with Paroxysmal or Persistent Atrial Fibrillation Following External Direct Current Electrical Cardioversion.Biomedicines. 2023 May 16;11(5):1452. doi: 10.3390/biomedicines11051452. Biomedicines. 2023. PMID: 37239123 Free PMC article. Review.
-
miR-486-5p diagnosed atrial fibrillation, predicted the risk of left atrial fibrosis, and regulated angiotensin II-induced cardiac fibrosis via modulating PI3K/Akt signaling through targeting FOXO1.Mol Cell Biochem. 2025 Feb;480(2):1077-1087. doi: 10.1007/s11010-024-05027-8. Epub 2024 May 23. Mol Cell Biochem. 2025. PMID: 38782834
References
-
- Packer DL, Kowal RC, Wheelan KR, Irwin JM, Champagne J, Guerra PG, et al. Cryoballoon ablation of pulmonary veins for paroxysmal atrial fibrillation: first results of the North American Arctic Front (STOP AF) pivotal trial. Journal of the American College of Cardiology. 2013;61(16):1713–1723. doi: 10.1016/j.jacc.2012.11.064. - DOI - PubMed
-
- Canpolat U, Oto A, Hazirolan T, Sunman H, Yorgun H, Sahiner L, et al. A prospective DE-MRI study evaluating the role of TGF-beta1 in left atrial fibrosis and implications for outcomes of cryoballoon-based catheter ablation: new insights into primary fibrotic atriocardiomyopathy. Journal of Cardiovascular Electrophysiology. 2015;26(3):251–259. doi: 10.1111/jce.12578. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials