

Anterolateral minithoracotomy versus median sternotomy for the surgical treatment of atrial septal defects: a meta-analysis and systematic review
- PMID: 34544460
- PMCID: PMC8451725
- DOI: 10.1186/s13019-021-01648-y
Anterolateral minithoracotomy versus median sternotomy for the surgical treatment of atrial septal defects: a meta-analysis and systematic review
Abstract
Background: To compare the short-term safety and efficacy of right anterolateral minithoracotomy (ALMT) and median sternotomy (MS) for the surgical treatment of atrial septal defects (ASDs).
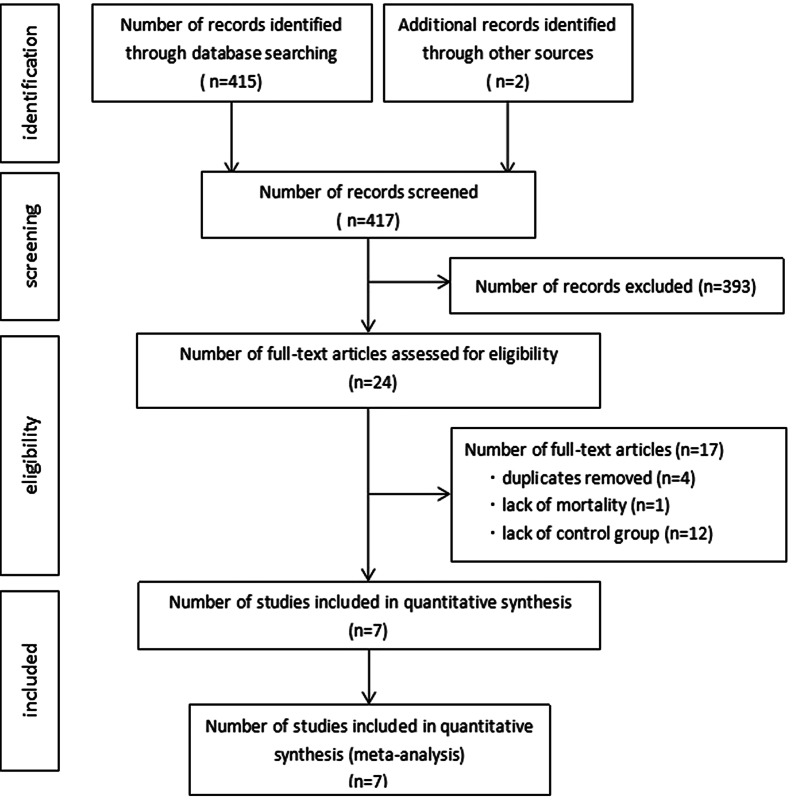
Methods: The PubMed, EMBASE, Web of Science, and Cochrane Library databases were searched for comparative studies focusing on surgical repair of ASDs via ALMT or MS published up to the end of April 27, 2020. We used random-effect or fixed-effect models to obtain pooled estimates.
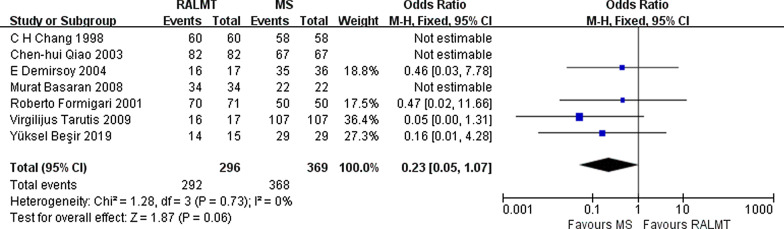
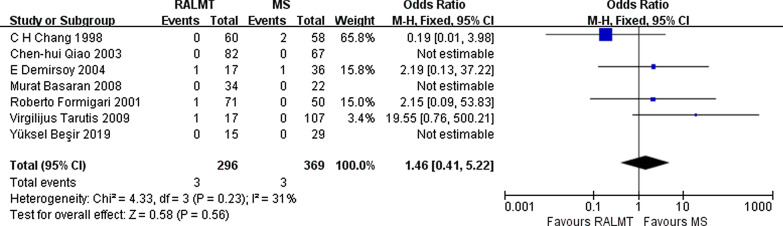
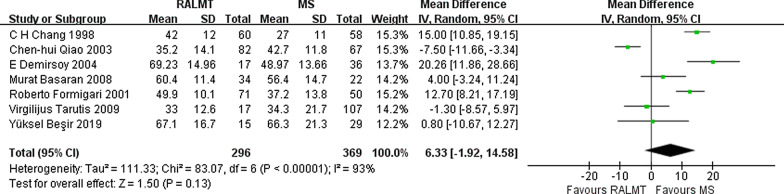
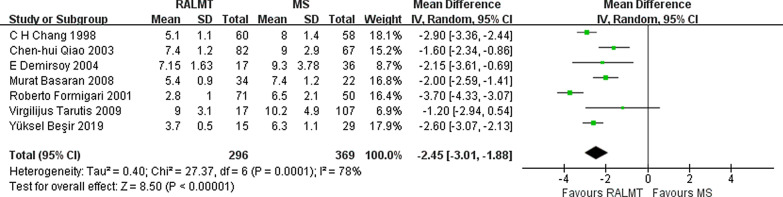
Results: A total of 7 publications, including 665 patients (ALMT 296 and MS 369), were included. Age (WMD: 1.80 years, 95% CI 0.31-3.29), weight (WMD: - 0.91 kg, 95% CI - 5.57 to 3.75), sex distribution (OR: 1.00, 95% CI 0.74-1.35) and surgical type (patch or direct closure) (OR: 1.00, 95% CI 0.67-1.49) were comparable in the ALMT group and MS group. No significant differences in the success rate (OR 0.23; 95% CI 0.05-1.07) or severe complication rate (OR 1.46; 95% CI 0.41-5.22) were found between the ALMT group and the MS group. In addition, the differences in the cardiopulmonary bypass (CPB) time (WMD 6.33; 95% CI - 1.92 to 14.58 min, p = 0.13) and the operation time (WMD 5.23; 95% CI - 12.49 to 22.96 min, p = 0.56) between the ALMT group and the MS group were not statistically significant. However, the ALMT group had a significantly longer aortic cross-clamp time (2.37 min more, 95% CI 1.07-3.67 min, p = 0.0003). The intubation time was 1.82 h shorter (95% CI - 3.10 to - 0.55 h; p = 0.005), the intensive care unit (ICU) stay was 0.24 days shorter (95% CI - 0.44 to - 0.04 days; p = 0.02), and the postoperative hospital stay was 2.45 days shorter (95% CI - 3.01 to - 1.88 days; p < 0.00001) in the ALMT group than in the MS group. Furthermore, the incision length was significantly shortened by 8.97 cm in the ALMT group compared with the MS group (95% CI - 9.36 to - 8.58 cm; p < 0.00001).
Conclusions: In the surgical treatment of ASD, ALMT and MS are equally safe and effective in terms of success rates and severe complication rates. The surgical procedures are equally difficult, but ALMT is associated with a faster functional recovery and better cosmetic results. Compared to MS, ALMT is the better choice for select ASD patients.
Keywords: Anterolateral minithoracotomy; Atrial septal defects; Median sternotomy; Meta-analysis; Surgery.
© 2021. The Author(s).
Conflict of interest statement
All authors declare that they have no competing interests.
Figures





References
-
- Butera G, Biondi-Zoccai G, Sangiorgi G, Abella R, Giamberti A, Bussadori C, Sheiban I, Saliba Z, Santoro T, Pelissero G, Carminati M, Frigiola A. Percutaneous versus surgical closure of secundum atrial septal defects: a systematic review and meta-analysis of currently available clinical evidence. Euro Interv. 2011;7(3):377–385. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
