

Incidence, Predictor, and Clinical Outcomes of Multiple Resheathing With Self-Expanding Valves During Transcatheter Aortic Valve Replacement
- PMID: 34546114
- PMCID: PMC8649510
- DOI: 10.1161/JAHA.120.020682
Incidence, Predictor, and Clinical Outcomes of Multiple Resheathing With Self-Expanding Valves During Transcatheter Aortic Valve Replacement
Abstract
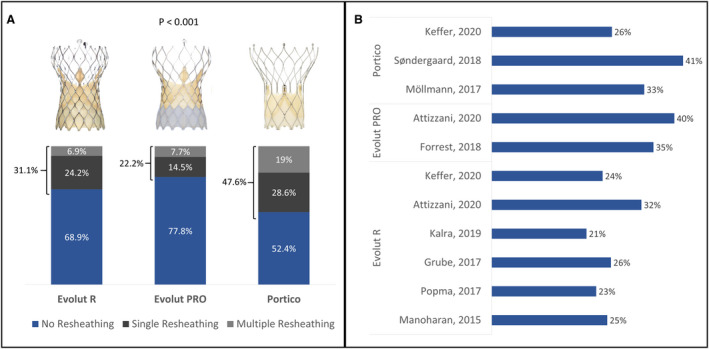
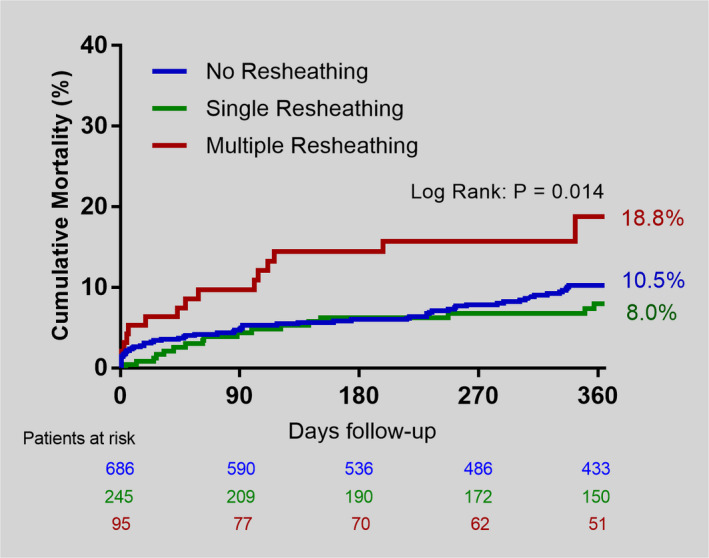
Background No study has evaluated the impact of the additional manipulation demanded by multiple resheathing (MR) in patients undergoing transcatheter aortic valve replacement with repositionable self-expanding valves. Methods and Results This study included a real-world, multicenter registry involving 16 centers from Canada, Germany, Latin America, and Spain. All consecutive patients who underwent transcatheter aortic valve replacement with the Evolut R, Evolut PRO, and Portico valves were included. Patients were divided according to the number of resheathing: no resheathing, single resheathing (SR), and MR. The primary end point was device success. Secondary outcomes included procedural complications, early safety events, and 1-year mortality. In 1026 patients, the proportion who required SR and MR was 23.9% and 9.3%, respectively. MR was predicted by the use of Portico and moderate/severe aortic regurgitation at baseline (both with P<0.01). Patients undergoing MR had less device success (no resheathing=89.9%, SR=89.8%, and MR=80%; P=0.01), driven by more need for a second prosthesis and device embolization. At 30 days, there were no differences in safety events. At 1 year, more deaths occurred with MR (no resheathing=10.5%, SR=8.0%, and MR=18.8%; P=0.014). After adjusting for baseline differences and center experience by annual volume, MR associated with less device success (odds ratio, 0.42; P=0.003) and increased 1-year mortality (hazard ratio, 2.06; P=0.01). When including only the Evolut R/PRO cases (N=837), MR continued to have less device success (P<0.001) and a trend toward increased mortality (P=0.05). Conclusions Repositioning a self-expanding valve is used in a third of patients, being multiple in ≈10%. MR, but not SR, was associated with more device failure and higher 1-year mortality, regardless of the type of valve implanted.
Keywords: aortic valve stenosis; resheathing; self‐expanding valve; transcatheter aortic valve replacement.
Conflict of interest statement
Dr Rodés‐Cabau has received institutional research grants from Medtronic (significant), Edwards Lifesciences (significant), and Boston Scientific (significant). Dr Ribeiro has served as proctor for Edwards Lifescience, Medtronic, and Boston Scientific (significant). Dr Nombela‐Franco has served as proctor for Abbott (significant) and has received speaker honoraria from Edwards Lifesciences (modest). Dr Amat Santos is proctor for Boston Scientific (significant) and has received institutional research grants from Medtronic, Abbott, and Boston Scientific (significant). Dr Mangione has served as proctor for Edwards Lifescience and Medtronic (modest). Dr Pessoa de Melo has served as proctor for Medtronic (significant). Dr Tumeleiro has served as proctor for Medtronic (significant). The remaining authors have no disclosures to report.
Figures
Comment in
-
Resheathing and Repositioning During Transcatheter Aortic Valve Implantation.J Am Heart Assoc. 2021 Sep 21;10(18):e022933. doi: 10.1161/JAHA.121.022933. Epub 2021 Sep 3. J Am Heart Assoc. 2021. PMID: 34476980 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
