

Preterm birth among women with and without severe acute respiratory syndrome coronavirus 2 infection
- PMID: 34546577
- PMCID: PMC8652761
- DOI: 10.1111/aogs.14269
Preterm birth among women with and without severe acute respiratory syndrome coronavirus 2 infection
Abstract
Introduction: Studies directly comparing preterm birth rates in women with and without severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection are limited. Our objective was to determine whether preterm birth was affected by SARS-CoV-2 infection within a large integrated health system in New York with a universal testing protocol.
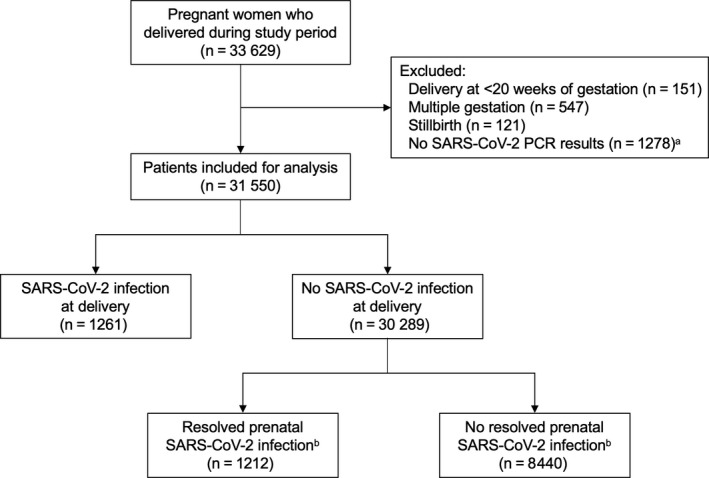
Material and methods: This retrospective cohort study evaluated data from seven hospitals in New York City and Long Island between March 2020 and June 2021, incorporating both the first and second waves of the coronavirus disease 2019 (COVID-19) pandemic in the USA. All patients with live singleton gestations who had SARS-CoV-2 polymerase chain reaction (PCR) testing at delivery were included. Deliveries before 20 weeks of gestation were excluded. The rate of preterm birth (before 37 weeks) was compared between patients with positive and negative SARS-CoV-2 test results. This analysis was performed separately for resolved prenatal infections and infections at delivery, with the latter group subdivided by symptom status. Multiple logistic regression analysis was used to examine the association between SARS-CoV-2 infection and preterm birth, adjusting for maternal age, race-ethnicity, parity, history of preterm birth, body mass index, marital status, insurance type, medical co-morbidities, month of delivery, and wave of pandemic.
Results: A total of 31 550 patients were included and 2473 (7.8%) had laboratory-confirmed infection. Patients with symptomatic COVID-19 at delivery were more likely to deliver preterm (19.0%; adjusted odds ratio 2.76, 95% CI 1.92-3.88) compared with women with asymptomatic infection (8.8%) or without infection (7.1%). Among preterm births associated with symptomatic infection, 72.5% were medically indicated compared with 44.1% among women without infection (p < 0.001). Risk of preterm birth in patients with resolved prenatal infection was unchanged when compared with women without infection. Among women with infection at delivery, preterm birth occurred more frequently during the second wave compared with the first wave (13.6% vs. 8.7%, respectively; p < 0.006). However, this was not significant on multiple regression analysis after adjusting for other explanatory variables.
Conclusions: Pregnant women with symptomatic COVID-19 are more than twice as likely to have a preterm delivery than patients without infection. Asymptomatic infection and resolved prenatal infection are not associated with increased risk.
Keywords: antibodies; coronavirus disease 2019; pregnancy; prematurity; preterm birth; race-ethnicity; severe acute respiratory syndrome coronavirus 2.
© 2021 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
None.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
