

Efficacy and Safety of Patritumab Deruxtecan (HER3-DXd) in EGFR Inhibitor-Resistant, EGFR-Mutated Non-Small Cell Lung Cancer
- PMID: 34548309
- PMCID: PMC9401524
- DOI: 10.1158/2159-8290.CD-21-0715
Efficacy and Safety of Patritumab Deruxtecan (HER3-DXd) in EGFR Inhibitor-Resistant, EGFR-Mutated Non-Small Cell Lung Cancer
Erratum in
-
Correction: Efficacy and Safety of Patritumab Deruxtecan (HER3-DXd) in EGFR Inhibitor-Resistant, EGFR-Mutated Non-Small Cell Lung Cancer.Cancer Discov. 2022 Jun 2;12(6):1598. doi: 10.1158/2159-8290.CD-22-0365. Cancer Discov. 2022. PMID: 35652222 Free PMC article. No abstract available.
Abstract
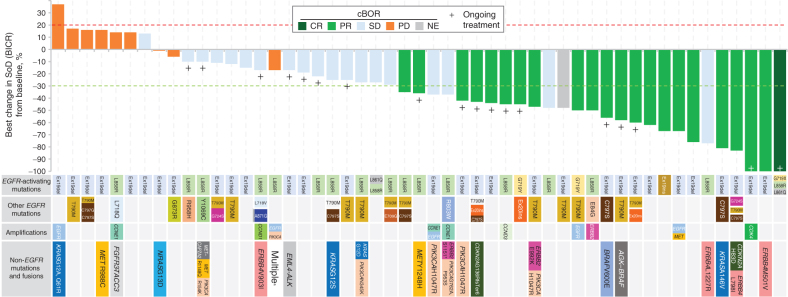
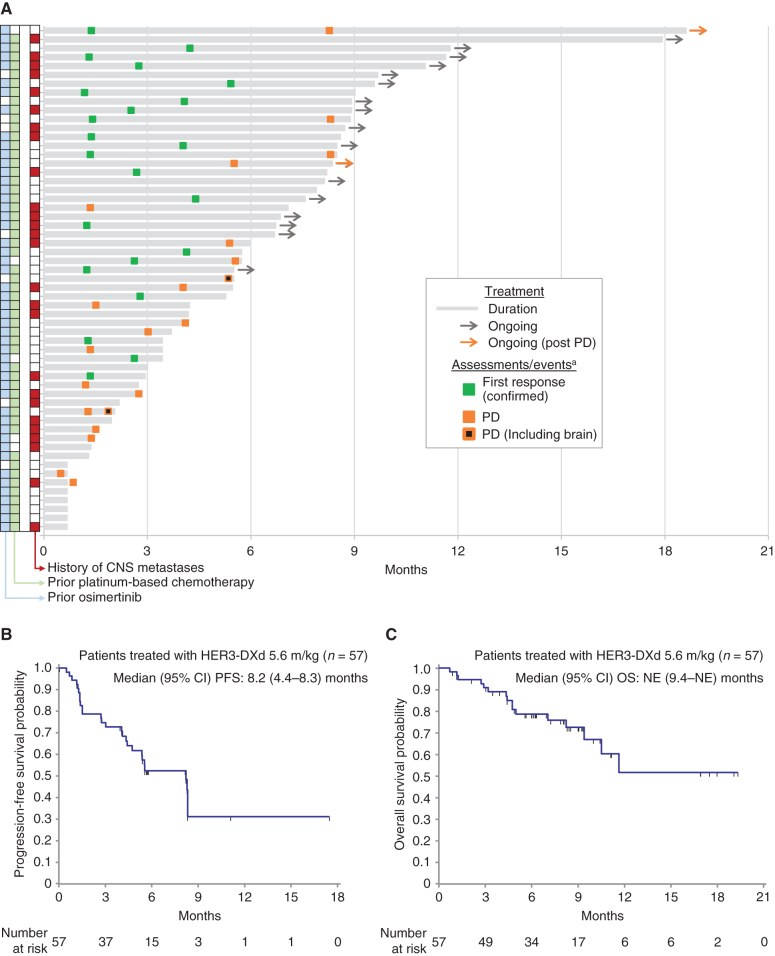
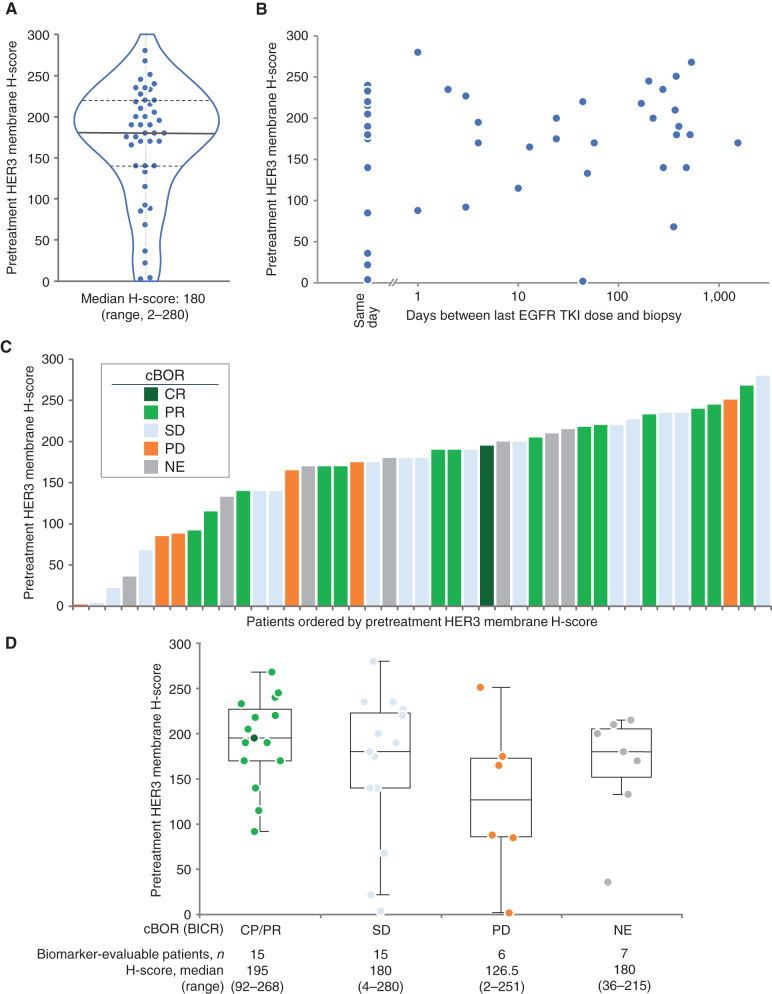
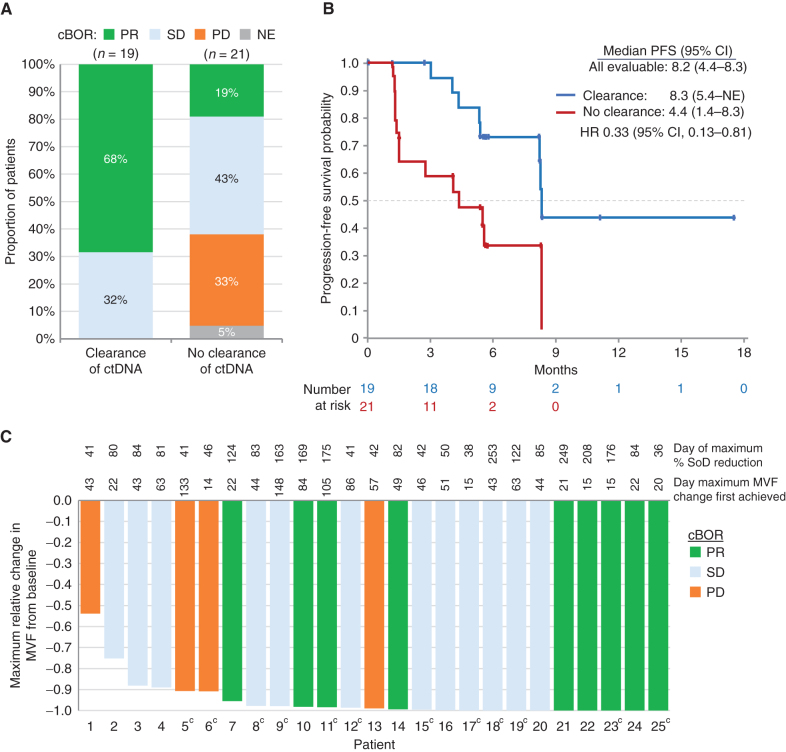
Receptor tyrosine-protein kinase ERBB3 (HER3) is expressed in most EGFR-mutated lung cancers but is not a known mechanism of resistance to EGFR inhibitors. HER3-DXd is an antibody-drug conjugate consisting of a HER3 antibody attached to a topoisomerase I inhibitor payload via a tetrapeptide-based cleavable linker. This phase I, dose escalation/expansion study included patients with locally advanced or metastatic EGFR-mutated non-small cell lung cancer (NSCLC) with prior EGFR tyrosine kinase inhibitor (TKI) therapy. Among 57 patients receiving HER3-DXd 5.6 mg/kg intravenously once every 3 weeks, the confirmed objective response rate by blinded independent central review (Response Evaluation Criteria in Solid Tumors v1.1) was 39% [95% confidence interval (CI), 26.0-52.4], and median progression-free survival was 8.2 (95% CI, 4.4-8.3) months. Responses were observed in patients with known and unknown EGFR TKI resistance mechanisms. Clinical activity was observed across a broad range of HER3 membrane expression. The most common grade ≥3 treatment-emergent adverse events were hematologic toxicities. HER3-DXd has clinical activity in EGFR TKI-resistant cancers independent of resistance mechanisms, providing an approach to treat a broad range of drug-resistant cancers. SIGNIFICANCE: In metastatic EGFR-mutated NSCLC, after disease progression on EGFR TKI therapy, treatment approaches include genotype-directed therapy targeting a known resistance mechanism or chemotherapy. HER3-DXd demonstrated clinical activity spanning known and unknown EGFR TKI resistance mechanisms. HER3-DXd could present a future treatment option agnostic to the EGFR TKI resistance mechanism.See related commentary by Lim et al., p. 16.This article is highlighted in the In This Issue feature, p. 1.
©2021 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
-
Patritumab Deruxtecan: Paving the Way for EGFR-TKI-Resistant NSCLC.Cancer Discov. 2022 Jan;12(1):16-19. doi: 10.1158/2159-8290.CD-21-1429. Cancer Discov. 2022. PMID: 35022206
References
-
- Soria JC, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KHet al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med 2018;378:113–25. - PubMed
-
- Ramalingam SS, Vansteenkiste J, Planchard D, Cho BC, Gray JE, Ohe Yet al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med 2020;382:41–50. - PubMed
-
- Rebuzzi SE, Alfieri R, La Monica S, Minari R, Petronini PG, Tiseo M. Combination of EGFR-TKIs and chemotherapy in advanced EGFR mutated NSCLC: review of the literature and future perspectives. Crit Rev Oncol Hematol 2020;146:102820. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
