

Association of biomarkers related to preoperative inflammatory and coagulation with postoperative in-hospital deaths in patients with type A acute aortic dissection
- PMID: 34548604
- PMCID: PMC8455536
- DOI: 10.1038/s41598-021-98298-w
Association of biomarkers related to preoperative inflammatory and coagulation with postoperative in-hospital deaths in patients with type A acute aortic dissection
Abstract
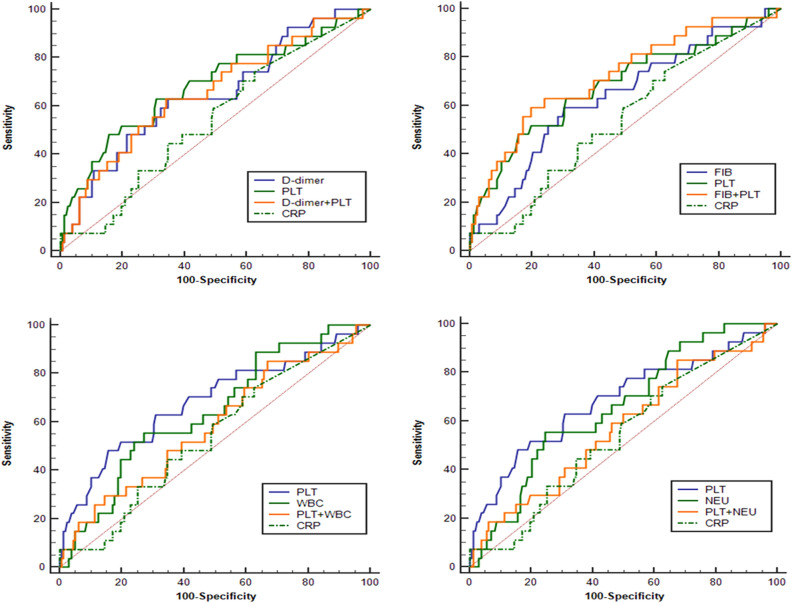
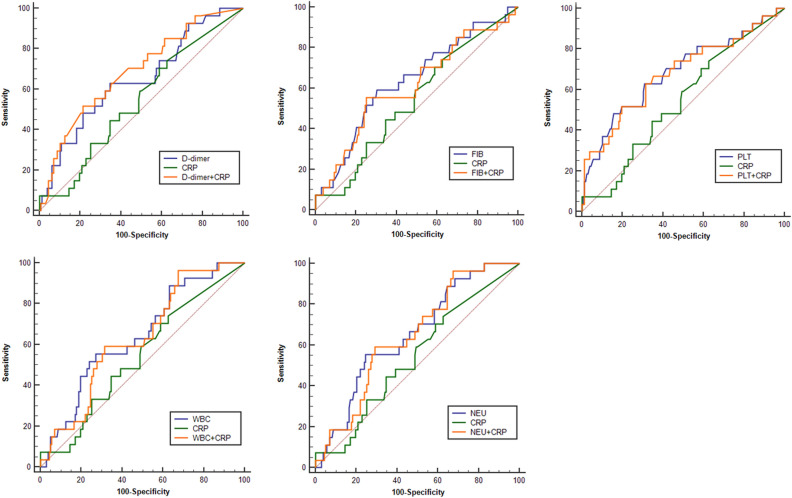
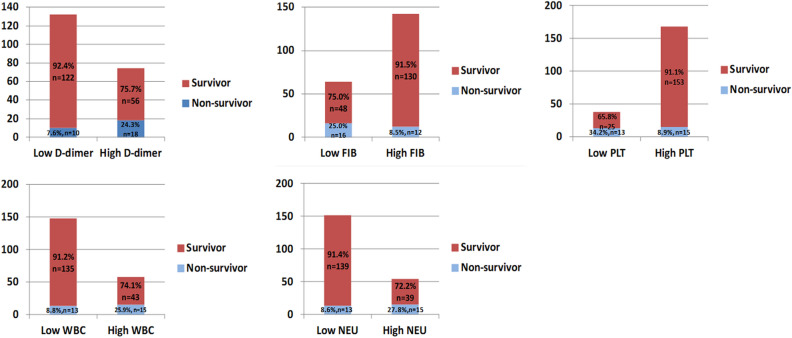
The aim of this study was to analyze the role of blood biomarkers regarding preoperative inflammation and coagulation in predicting the postoperative in-hospital mortality of patients with type A acute aortic dissection (AAD). A total of 206 patients with type A AAD who had received surgical treatment were enrolled in this study. Patients were divided into two groups: the death group (28 patients who died during hospitalization) and the survival group (178 patients). Peripheral blood samples were collected before anesthesia induction. Preoperative levels of D-dimer, fibrinogen (FIB), platelet (PLT), white blood cells (WBC) and neutrophil (NEU) were compared between the two groups. Univariable and multivariable logistic regression analysis were utilized to identify the independent risk factors for postoperative in-hospital deaths of patients with type A AAD. Receiver operating characteristic (ROC) curve were used to analyze the predictive value of these indices in the postoperative in-hospital mortality of the patients. Univariable logistic regression analysis showed that the P values of the five parameters including D-dimer, FIB, PLT, WBC and NEU were all less than 0.1, which may be risk factors for postoperative in-hospital deaths of patients with type A AAD. Further multivariable logistic regression analysis indicated that higher preoperative D-dimer and WBC levels were independent risk factors for postoperative in-hospital mortality of patients with type A AAD. ROC curve analysis indicated that application of combining FIB and PLT could improve accuracy in prediction of postoperative in-hospital mortality in patients with type A AAD. Both preoperative D-dimer and WBC in patients with type A AAD may be used as independent risk factors for the postoperative in-hospital mortality of such patients. The combination of FIB and PLT may improve the accuracy of clinical prognostic assessment.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Evangelista A, Isselbacher EM, Bossone E, Gleason TG, Eusanio MD, Sechtem U, Ehrlich MP, Trimarchi S, Braverman AC, Myrmel T, Harris KM, Hutchinson S, O'Gara P, Suzuki T, Nienaber CA, Eagle KA, Investigators I. Insights from the international registry of acute aortic dissection: A 20-year experience of collaborative clinical research. Circulation. 2018;137:1846–1860. doi: 10.1161/CIRCULATIONAHA.117.031264. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
