

Vertical and horizontal ridge augmentation using customized CAD/CAM titanium mesh with versus without resorbable membranes. A randomized clinical trial
- PMID: 34551168
- PMCID: PMC9293224
- DOI: 10.1111/clr.13841
Vertical and horizontal ridge augmentation using customized CAD/CAM titanium mesh with versus without resorbable membranes. A randomized clinical trial
Abstract
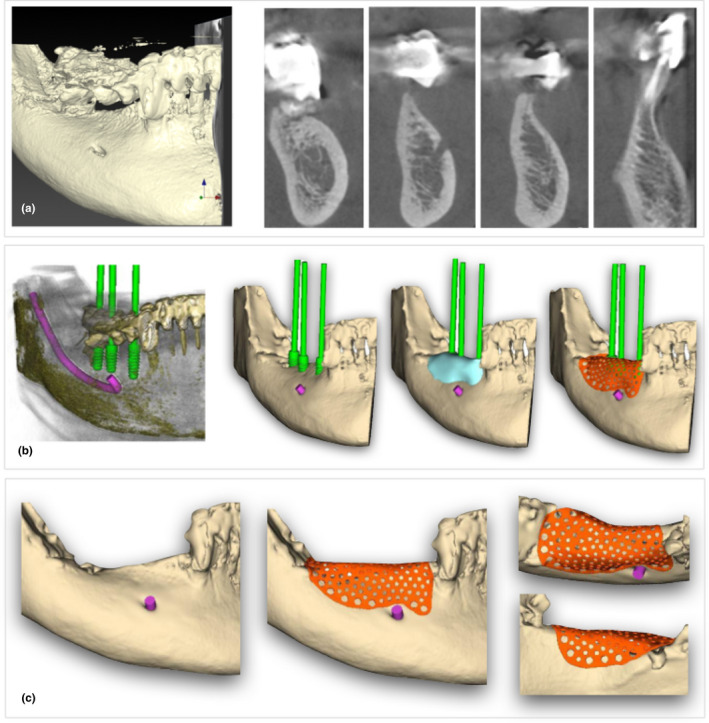
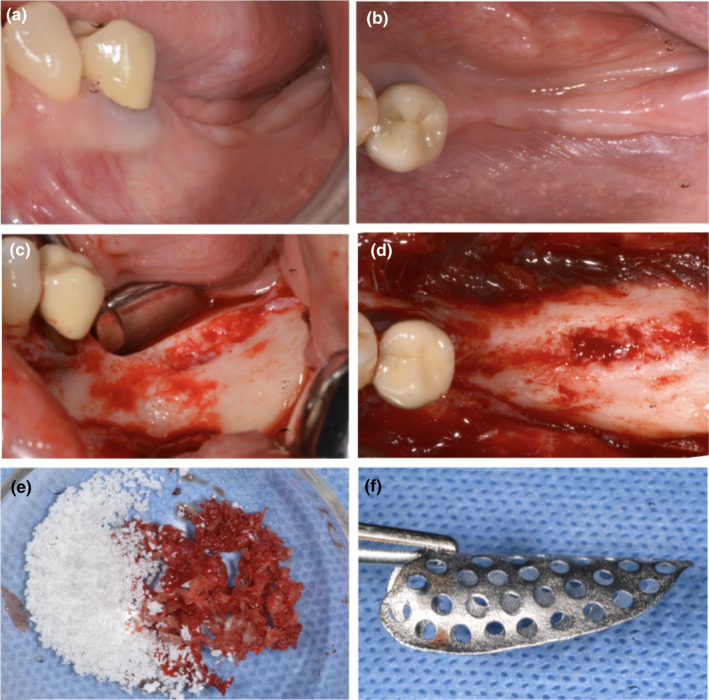
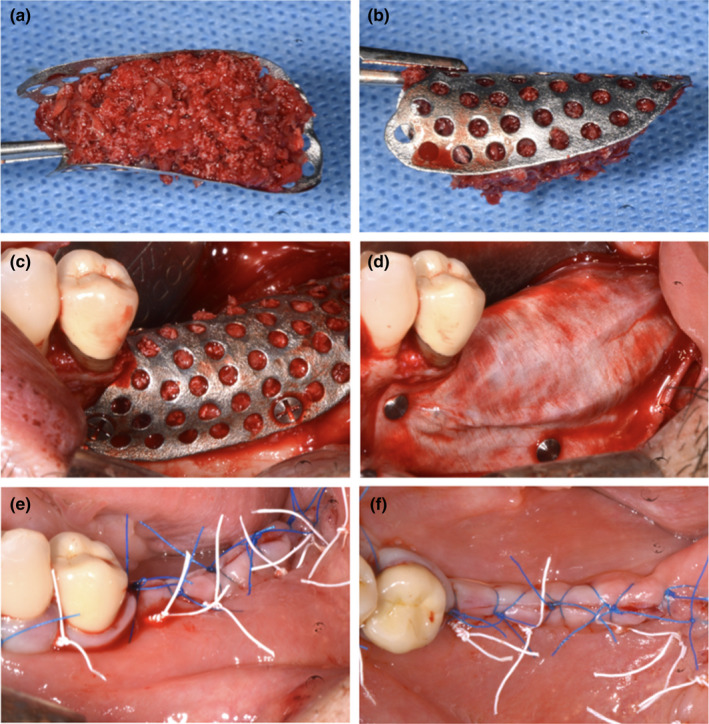
Objectives: The aim was to evaluate the role of resorbable membranes applied over customized titanium meshes related to soft tissue healing and bone regeneration after vertical/horizontal bone augmentation.
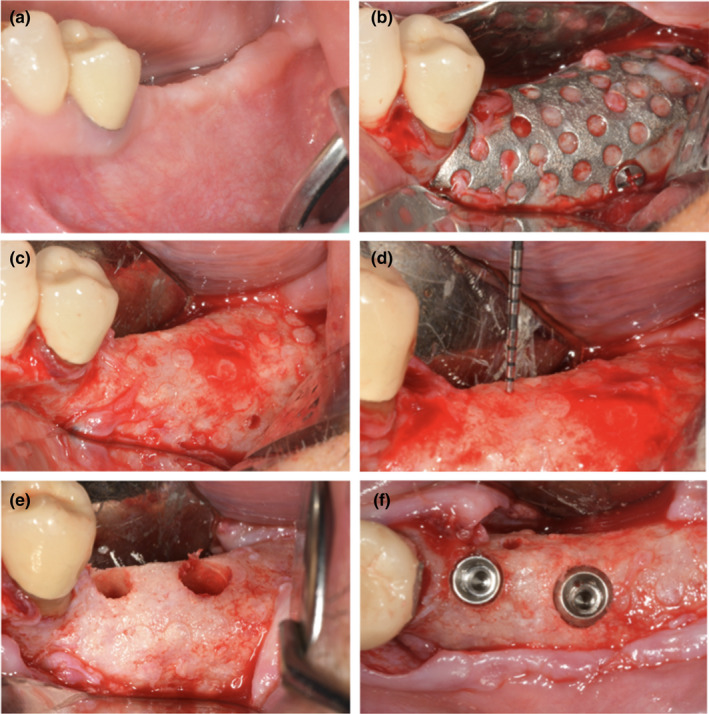
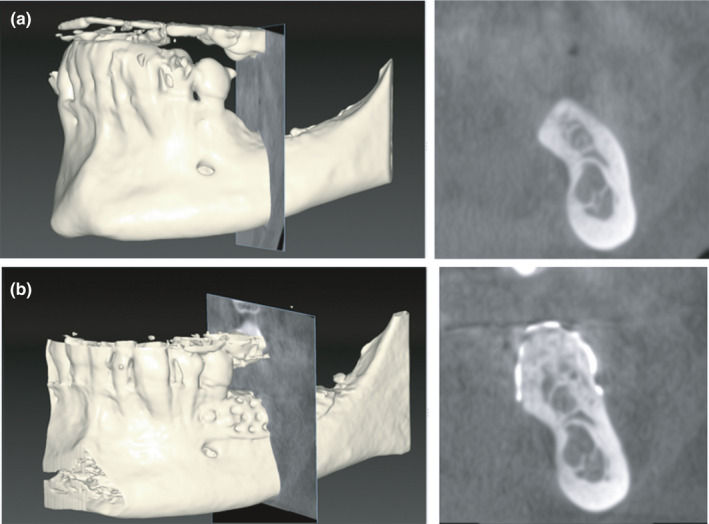
Materials and methods: Thirty patients with partial edentulism of the maxilla/mandible, with vertical/horizontal reabsorption of the alveolar bone, and needing implant-supported restorations, were randomly divided into two groups: Group A was treated using only custom-made meshes (Mesh-) and Group B using custom-made meshes with cross-linked collagen membranes (Mesh+). Data collection included surgical/technical and healing complications, "pseudo-periosteum" thickness, bone density, planned bone volume (PBV), regenerated bone volume (RBV), regeneration rate (RR), vertical bone gain (VBG), and implant survival in regenerated areas. Statistical analysis was performed between the two study groups using a significance level of α = .05.
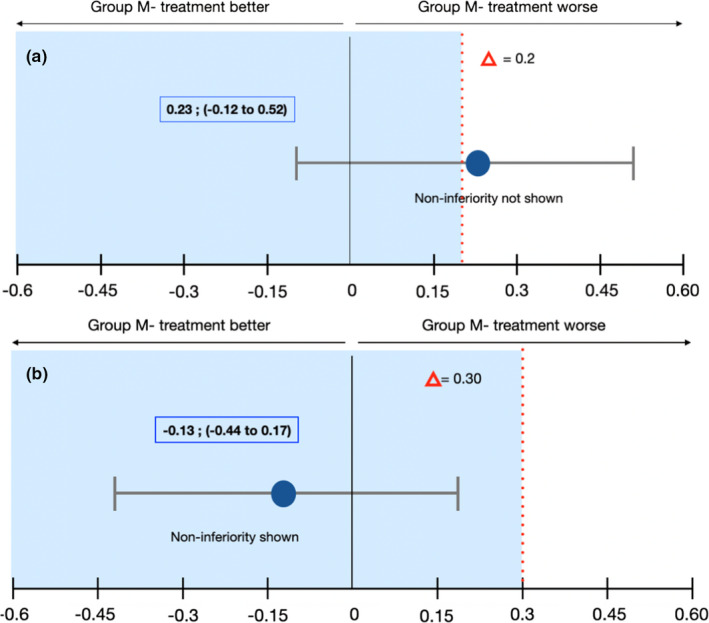
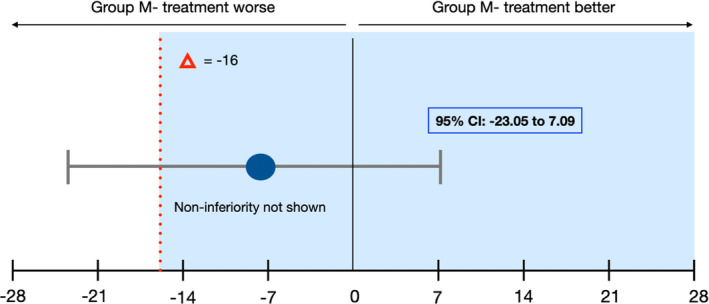
Results: Regarding the healing complications, the noninferiority analysis proved to be inconclusive, despite the better results of group Mesh+ (13%) compared to group Mesh- (33%): estimated value -1.13 CI-95% from -0.44 to 0.17. Superiority approach confirmed the absence of significant differences (p = .39). RBV was 803.27 mm3 and 843.13 mm3 , respectively, and higher RR was observed in group Mesh+ (82.3%) compared to Mesh- (74.3%), although this value did not reach a statistical significance (p = .44). All 30 patients completed the study, receiving 71 implants; 68 out of them were clinically stable and in function.
Conclusion: The results showed that customized meshes alone do not appear to be inferior to customized meshes covered by cross-linked collagen membranes in terms of healing complication rates and regeneration rates, although superior results were observed in group Mesh+compared to group Mesh- for all variables.
Keywords: alveolar ridge augmentation; collagen membrane; healing complication; osseointegrated implants; titanium mesh.
© 2021 The Authors. Clinical Oral Implants Research published by John Wiley & Sons Ltd.
Figures
References
-
- Alayan, J. , & Ivanovski, S. (2018). A prospective controlled trial comparing xenograft/autogenous bone and collagen‐stabilized xenograft for maxillary sinus augmentation‐complications, patient‐reported outcomes and volumetric analysis. Clinical Oral Implants Research, 29(2), 248–262. 10.1111/clr.13107 - DOI - PubMed
-
- Bornstein, M. M. , Al‐Nawas, B. , Kuchler, U. , & Tahmaseb, A. (2014). Consensus statements and recommended clinical procedures regarding contemporary surgical and radiographic techniques in implant dentistry. The International Journal of Oral & Maxillofacial Implants, 29S, 78–82. 10.11607/jomi.2013.g1 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
