

Acute Closed-Angle Glaucoma-an Ophthalmological Emergency
- PMID: 34551857
- PMCID: PMC8841641
- DOI: 10.3238/arztebl.m2021.0264
Acute Closed-Angle Glaucoma-an Ophthalmological Emergency
Abstract
Background: Acute closed-angle glaucoma has an incidence of 2.2-4.1 cases per 100 000 persons per year in Europe. It is an ophthalmological emergency in which markedly elevated intraocular pressure can damage vision permanently. Because the acute symptoms are not always clearly referable to the eyes, patients often present to physicians who are not ophthalmologists.
Methods: This review is based on pertinent articles retrieved by a selective search in PubMed.
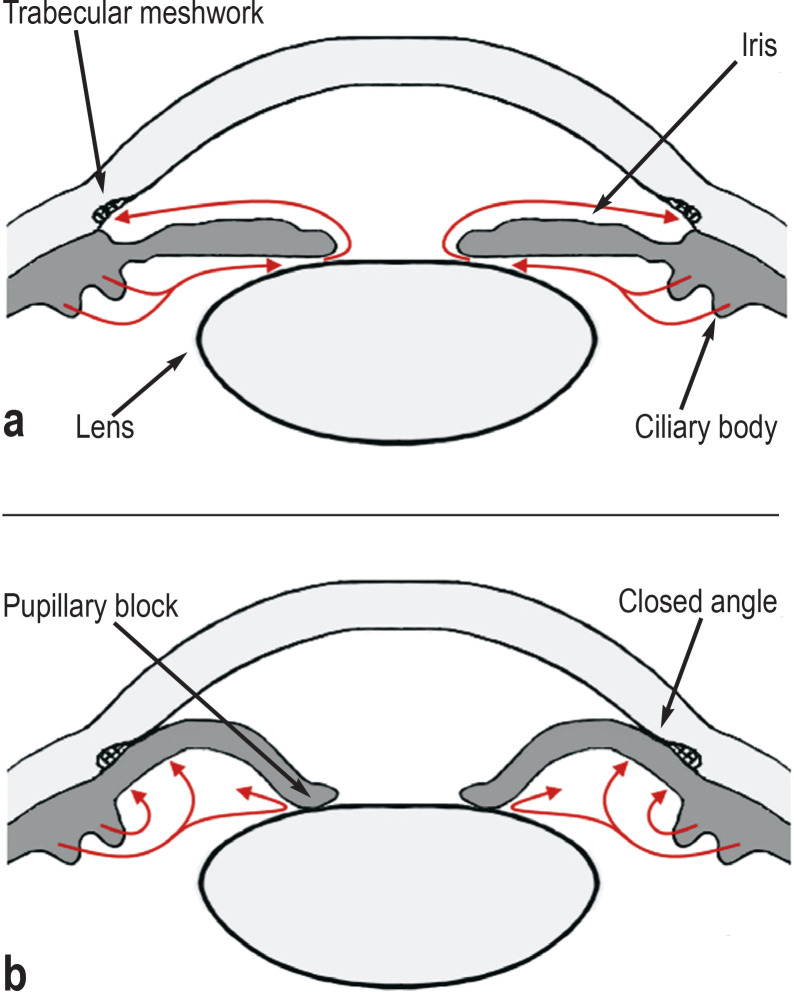
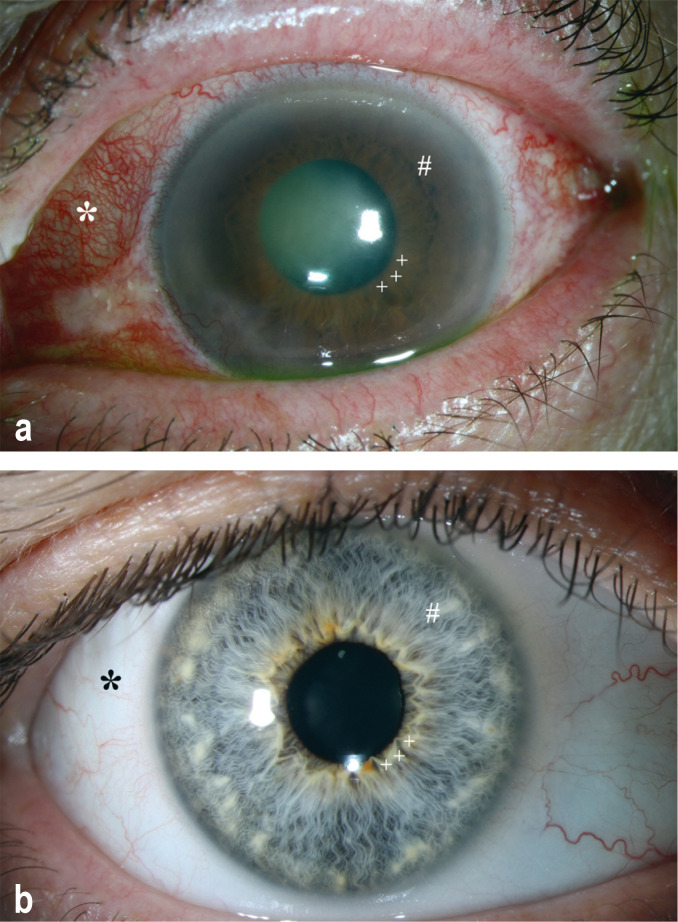
Results: The diverse symptoms of acute closed-angle glaucoma include eye redness, worsening of vision and other visual disturbances, headache, and nausea. Acute closed-angle glaucoma has multiple causes. Not all predisposing factors have been definitively identified; above all, there are certain anatomical configurations of the eye that make it more likely to arise. The goals of treatment are to reduce the elevated intraocular pressure rapidly, which usually leads to marked symptom relief, as well as to eliminate the situation that led to closed-angle glaucoma. For proper treatment, the patient should be seen by an ophthalmologist without delay, on the day of symptom onset if possible.
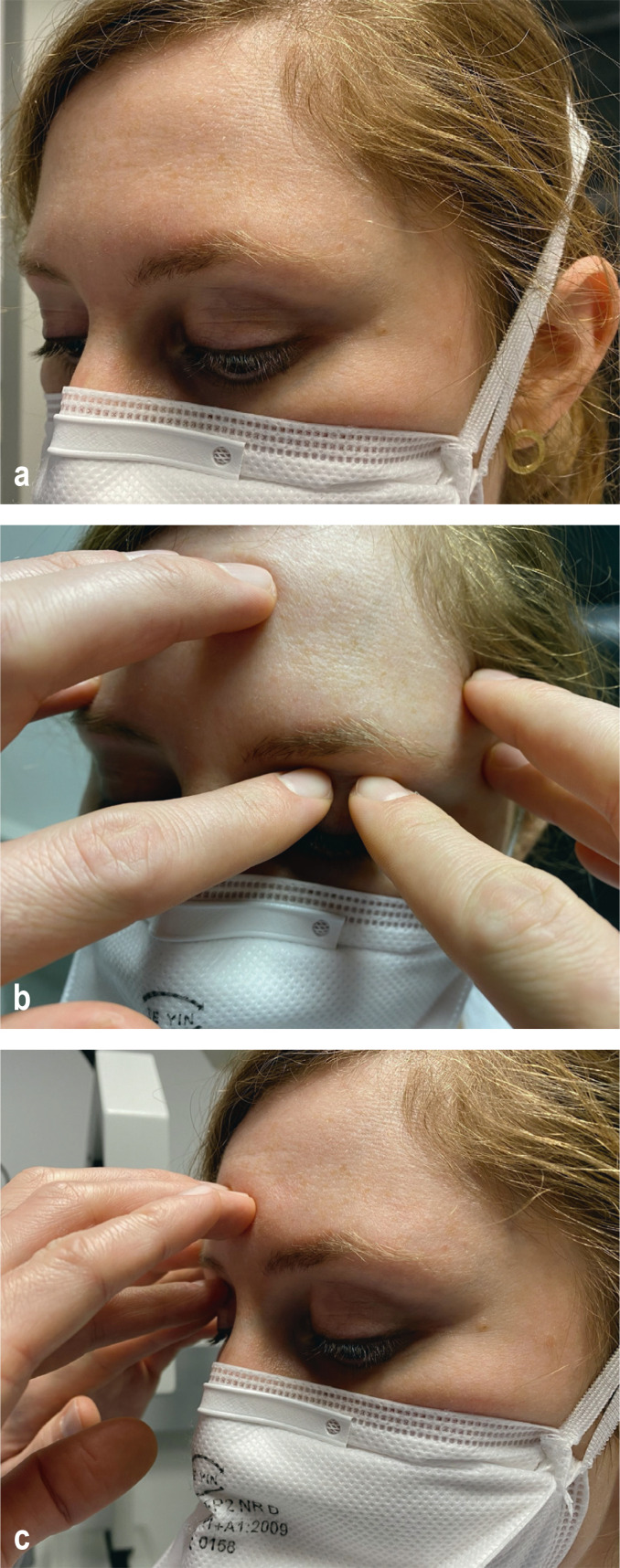
Conclusion: Primary prevention of acute closed-angle glaucoma is not always possible. Even physicians who are not ophthalmologists can diagnose markedly elevated intraocular pressure by palpation of the globe. Proper, specific treatment can help patients rapidly and lastingly.
Figures
Comment in
-
Causual Effects of Mydriatic Eye Drops.Dtsch Arztebl Int. 2022 May 13;119(19):352. doi: 10.3238/arztebl.m2022.0095. Dtsch Arztebl Int. 2022. PMID: 35974463 Free PMC article. No abstract available.
-
In Reply.Dtsch Arztebl Int. 2022 May 13;119(19):352. doi: 10.3238/arztebl.m2022.0096. Dtsch Arztebl Int. 2022. PMID: 35974464 Free PMC article. No abstract available.
References
-
- Prum BE, Herndon LW, Moroi SE, et al. Primary angle closure preferred practice pattern®. Guidelines. Ophthalmology. 2016;123:1–40. - PubMed
-
- Ramesh S, Maw C, Sutton CJ, Gandhewar JR, Kelly SP. Ethnic aspects of acute primary angle closure in a UK mulicultural conurbation. Eye (Lond) 2005;19:1271–1275. - PubMed
-
- Chua PY, Day AC, Lai KL, et al. The incidence of acute angle closure in Scotland: a prospective surveillance study. Br J Ophthalmol. 2018;102:539–543. - PubMed
-
- David R, Tessler Z, Yassur Y. Epidemiology of acute angle-closure glaucoma: incidence and seasonal variations. Ophthalmologica. 1985;191:4–7. - PubMed
LinkOut - more resources
Full Text Sources