

Anti-Ro/SSA Antibodies and the Autoimmune Long-QT Syndrome
- PMID: 34552948
- PMCID: PMC8450397
- DOI: 10.3389/fmed.2021.730161
Anti-Ro/SSA Antibodies and the Autoimmune Long-QT Syndrome
Abstract
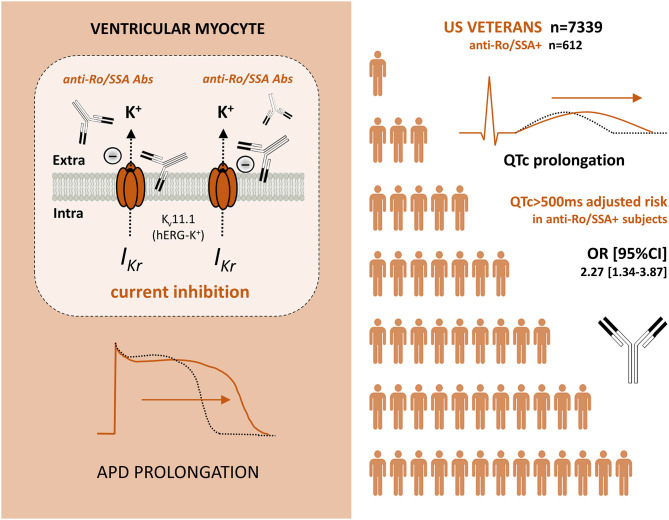
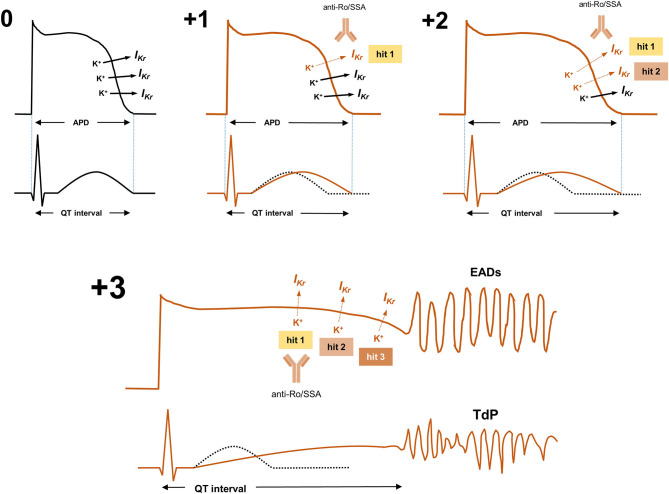
Autoimmunity is increasingly recognized as a novel pathogenic mechanism for cardiac arrhythmias. Several arrhythmogenic autoantibodies have been identified, cross-reacting with different types of surface proteins critically involved in the cardiomyocyte electrophysiology, primarily ion channels (autoimmune cardiac channelopathies). Specifically, some of these autoantibodies can prolong the action potential duration leading to acquired long-QT syndrome (LQTS), a condition known to increase the risk of life-threatening ventricular arrhythmias, particularly Torsades de Pointes (TdP). The most investigated form of autoimmune LQTS is associated with the presence of circulating anti-Ro/SSA-antibodies, frequently found in patients with autoimmune diseases (AD), but also in a significant proportion of apparently healthy subjects of the general population. Accumulating evidence indicates that anti-Ro/SSA-antibodies can markedly delay the ventricular repolarization via a direct inhibitory cross-reaction with the extracellular pore region of the human-ether-a-go-go-related (hERG) potassium channel, resulting in a higher propensity for anti-Ro/SSA-positive subjects to develop LQTS and ventricular arrhythmias/TdP. Recent population data demonstrate that the risk of LQTS in subjects with circulating anti-Ro/SSA antibodies is significantly increased independent of a history of overt AD, intriguingly suggesting that these autoantibodies may silently contribute to a number of cases of ventricular arrhythmias and cardiac arrest in the general population. In this review, we highlight the current knowledge in this topic providing complementary basic, clinical and population health perspectives.
Keywords: Torsades de Pointes; anti-Ro/SSA antibodies; autoimmune cardiac channelopathies; hERG potassium channel; long QT syndrome; sudden cardiac death.
Copyright © 2021 Lazzerini, Laghi-Pasini, Boutjdir and Capecchi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Drew BJ, Ackerman MJ, Funk M, Gibler WB, Kligfield P, Menon V, et al. . Prevention of torsade de pointes in hospital settings: a scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation. (2010) 121:1047–60. 10.1161/CIRCULATIONAHA.109.192704 - DOI - PMC - PubMed
-
- Drew BJ, Ackerman MJ, Funk M, Gibler WB, Kligfield P, Menon V, et al. . Prevention of torsade de pointes in hospital settings: a scientific statement from the American Heart Association and the American College of Cardiology Foundation. J Am Coll Cardiol. (2010) 55:934–47. 10.1016/j.jacc.2010.01.001 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials