

Development and validation of a polysocial risk score for atherosclerotic cardiovascular disease
- PMID: 34553187
- PMCID: PMC8441152
- DOI: 10.1016/j.ajpc.2021.100251
Development and validation of a polysocial risk score for atherosclerotic cardiovascular disease
Abstract
Objective: To date, the extent to which social determinants of health (SDOH) may help identify individuals with atherosclerotic cardiovascular disease (ASCVD) - beyond traditional risk factors - has not been quantified using a cumulative social disadvantage approach. The objective of this study was to develop, and validate, a polysocial risk score (PsRS) for prevalent ASCVD in a nationally representative sample of adults in the United States (US).
Methods: We used data from the 2013-2017 National Health Interview Survey. A total of 38 SDOH were identified from the database. Stepwise and criterion-based selection approaches were applied to derive PsRS, after adjusting for traditional risk factors. Logistic regression models were fitted to assign risk scores to individual SDOH, based on relative effect size magnitudes. PsRS was calculated by summing risk scores for individual SDOH, for each participant; and validated using a separate validation cohort.
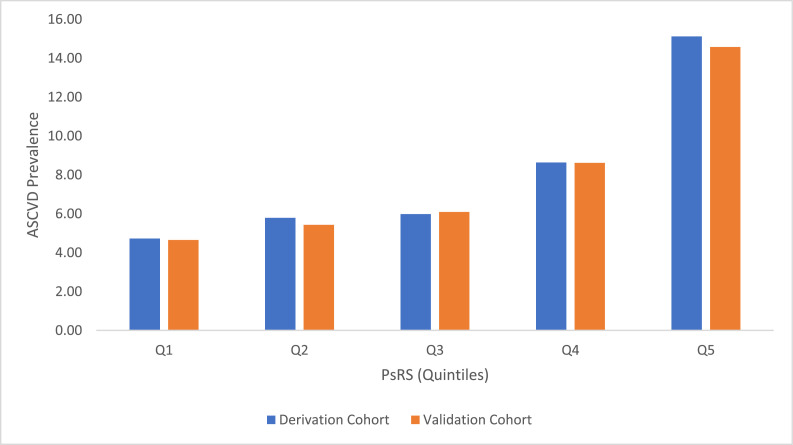
Results: Final sample comprised 164,696 adults. PsRS included 7 SDOH: unemployment, inability to pay medical bills, low income, psychological distress, delayed care due to lack of transport, food insecurity, and less than high school education. PsRS ranged from 0-20 and exhibited excellent calibration and discrimination. Individuals with the highest PsRS (5th quintile) had nearly 4-fold higher ASCVD prevalence, relative to those with the lowest risk scores (1st quintile). Area under receiver operating curve (AU-ROC) for PsRS with SDOH alone was 0.836. Addition of SDOH to the model with only demographic and clinical risk factors (AU-ROC=0.852) improved overall discriminatory power, with AU-ROC for final PsRS (demographics + clinical + SDOH) = 0.862.
Conclusions: Cumulatively, SDOH may help identify individuals with ASCVD, beyond traditional cardiovascular risk factors. In this study, we provide a unique validated PsRS for ASCVD in a national sample of US adults. Future study should target development of similar scores in diverse populations, and incorporate longitudinal study designs.
Keywords: ASCVD; ASCVD, atherosclerotic cardiovascular disease; Cardiovascular disease; Polysocial risk score; PsRS, polysocial risk score; SDOH, social determinants of health; Social determinants of health.
© 2021 The Authors. Published by Elsevier B.V.
Conflict of interest statement
Dr. Nasir is on the advisory board of Amgen (CA), Esperion (MI) and Novartis (NJ), and his research is partly supported by the Jerold B. Katz Academy of Translational Research (TX). No other conflicts of interest relevant to the content of this manuscript were reported by the authors. The funding source had no involvement in the preparation of this article.
Figures


References
-
- Marmot M, Friel S, Bell R, Houweling TA, Taylor S. Closing the gap in a generation: health equity through action on the social determinants of health. Lancet. 2008;372:1661–1669. - PubMed
-
- Lang T, Lepage B, Schieber A-C, Lamy S, Kelly-Irving M. Social determinants of cardiovascular diseases. Public Health Rev. 2011;33:601–622. 2011/12/01.
-
- Javed Z, Jilani H, Yahya T, Khan S, Dubey P, Hyder A, Cainzos-Achirica M, Kash BA, Nasir K. Social Determinants of cardiovascular disease: moving a step closer to health equity. precision medicine in cardiovascular disease prevention. In-Print.
-
- Stringhini S, Carmeli C, Jokela M, Avendaño M, Muennig P, Guida F, Ricceri F, d'Errico A, Barros H, Bochud M, Chadeau-Hyam M, Clavel-Chapelon F, Costa G, Delpierre C, Fraga S, Goldberg M, Giles GG, Krogh V, Kelly-Irving M, Layte R, Lasserre AM, Marmot MG, Preisig M, Shipley MJ, Vollenweider P, Zins M, Kawachi I, Steptoe A, Mackenbach JP, Vineis P, Kivimäki M. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1•7 million men and women. Lancet. 2017;389:1229–1237. - PMC - PubMed
-
- Diez Roux AV, Merkin SS, Arnett D, Chambless L, Massing M, Nieto FJ, Sorlie P, Szklo M, Tyroler HA, Watson RL. Neighborhood of residence and incidence of coronary heart disease. N Engl J Med. 2001;345:99–106. - PubMed
LinkOut - more resources
Full Text Sources
