

The Status of Adjuvant and Neoadjuvant Melanoma Therapy, New Developments and Upcoming Challenges
- PMID: 34554353
- PMCID: PMC8484171
- DOI: 10.1007/s11523-021-00840-3
The Status of Adjuvant and Neoadjuvant Melanoma Therapy, New Developments and Upcoming Challenges
Abstract
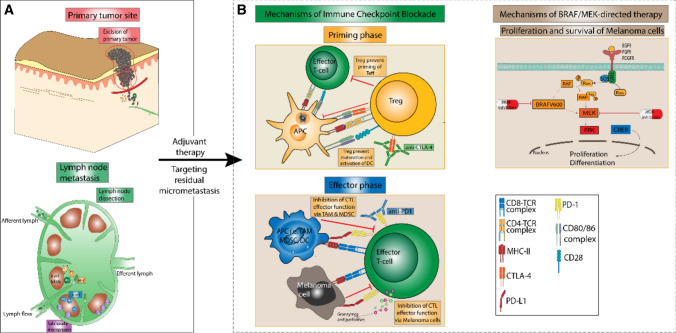
The global incidence of malignant melanoma, the leading cause of skin cancer death, has steadily increased in recent years. Surgical excision is the treatment of choice for early-stage melanoma. However, 40-60% of patients with high-risk melanoma or with nodal involvement eventually experience loco-regional relapse or tumor progression. Adjuvant therapy aims to reduce the rate of recurrence in radically operated high-risk patients with melanoma and thus improves survival. Interferon-α has long been the only approved drug for adjuvant melanoma therapy, despite an unclear survival benefit. The landmark success of immune-checkpoint inhibitors and BRAF/MEK-directed targeted therapies in the treatment of patients with stage IV melanoma led to the initiation of clinical trials in the adjuvant setting. These trials demonstrated the efficacy of immune-checkpoint inhibitors and targeted therapies for the adjuvant treatment of high-risk patients with melanoma, as shown both by an increase in recurrence-free survival and the emergence of long-term survivors, finally resulting in the approval of the cytotoxic T-lymphocyte antigen 4 inhibitor ipilimumab, PD1 inhibitors (nivolumab, pembrolizumab), and BRAF/MEK inhibitors for adjuvant melanoma therapy. This review aims to delineate the advances in adjuvant melanoma therapy, issuing particularly recent results from clinical trials. Moreover, we also discuss pending issues and future challenges, which comprise the adequate selection of adjuvant regimens for patient subgroups and the identification of markers likely to predict the individual response to adjuvant treatments. Last, we outline the role of emerging neoadjuvant approaches, which may complement adjuvant strategies and are currently investigated in clinical trials.
© 2021. The Author(s).
Conflict of interest statement
H.S., M.H., U.N., M.S., S.P., J.H., C.L., and S.G. declare that they have no conflicts of interest that might be relevant to the contents of this manuscript.
Figures

References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7–34. - PubMed
-
- Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. The Eighth edition AJCC Cancer Staging Manual: continuing to build a bridge from a population-based to a more "personalized" approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–99. - PubMed
-
- Karakousis CP, Balch CM, Urist MM, Ross MM, Smith TJ, Bartolucci AA. Local recurrence in malignant melanoma: long-term results of the multiinstitutional randomized surgical trial. Ann Surg Oncol. 1996;3(5):446–452. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
