

Chimeric antigen receptor (CAR) immunotherapy: basic principles, current advances, and future prospects in neuro-oncology
- PMID: 34554405
- PMCID: PMC8580929
- DOI: 10.1007/s12026-021-09236-x
Chimeric antigen receptor (CAR) immunotherapy: basic principles, current advances, and future prospects in neuro-oncology
Abstract
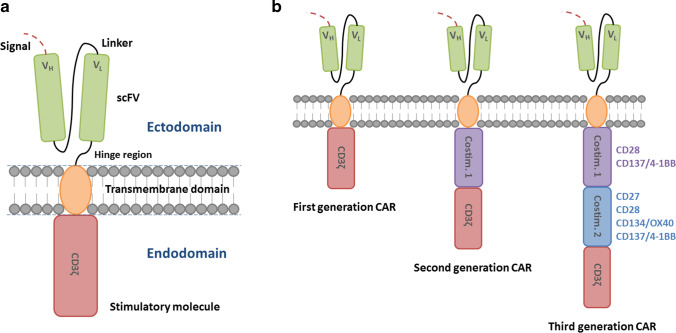
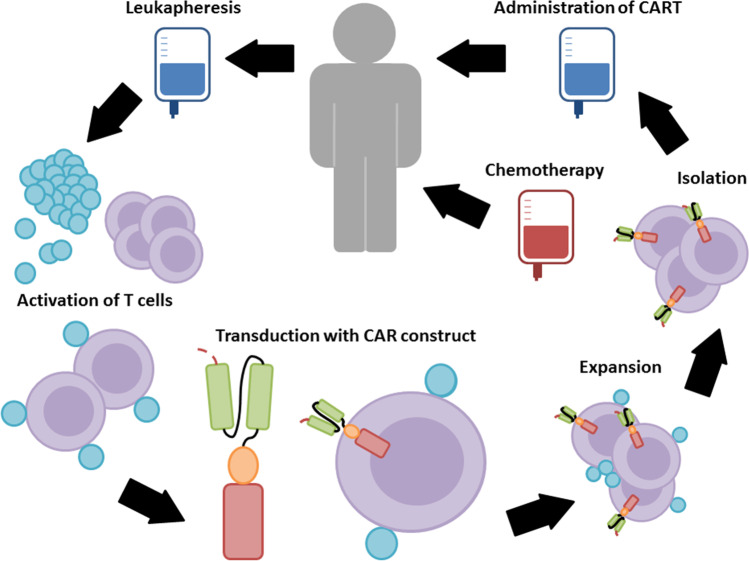
With recent advances, chimeric antigen receptor (CAR) immunotherapy has become a promising modality for patients with refractory cancer diseases. The successful results of CAR T cell therapy in relapsed and refractory B-cell malignancies shifted the paradigm of cancer immunotherapy by awakening the scientific, clinical, and commercial interest in translating this technology for the treatment of solid cancers. This review elaborates on fundamental principles of CAR T cell therapy (development of CAR construct, challenges of CAR T cell therapy) and its application on solid tumors as well as CAR T cell therapy potential in the field of neuro-oncology. Glioblastoma (GBM) is identified as one of the most challenging solid tumors with a permissive immunological milieu and dismal prognosis. Standard multimodal treatment using maximal safe resection, radiochemotherapy, and maintenance chemotherapy extends the overall survival beyond a year. Recurrence is, however, inevitable. GBM holds several unique features including its vast intratumoral heterogeneity, immunosuppressive environment, and a partially permissive anatomic blood-brain barrier, which offers a unique opportunity to investigate new treatment approaches. Tremendous efforts have been made in recent years to investigate novel CAR targets and target combinations with standard modalities for solid tumors and GBM to improve treatment efficacy. In this review, we outline the history of CAR immunotherapy development, relevant CAR target antigens validated with CAR T cells as well as preclinical approaches in combination with adjunct approaches via checkpoint inhibition, bispecific antibodies, and second-line systemic therapies that enhance anticancer efficacy of the CAR-based cancer immunotherapy.
Keywords: Adoptive cell therapy; CAR; Chimeric antigen receptor; Immunotherapy; Neuro-oncology; T cells.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
