

RAF1 amplification drives a subset of bladder tumors and confers sensitivity to MAPK-directed therapeutics
- PMID: 34554931
- PMCID: PMC8592548
- DOI: 10.1172/JCI147849
RAF1 amplification drives a subset of bladder tumors and confers sensitivity to MAPK-directed therapeutics
Abstract
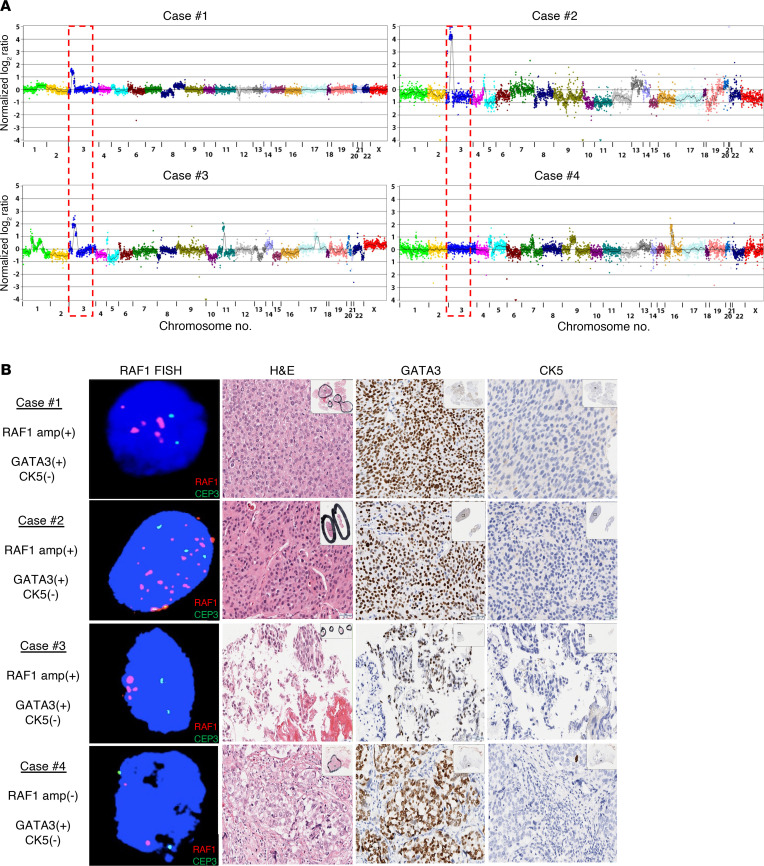
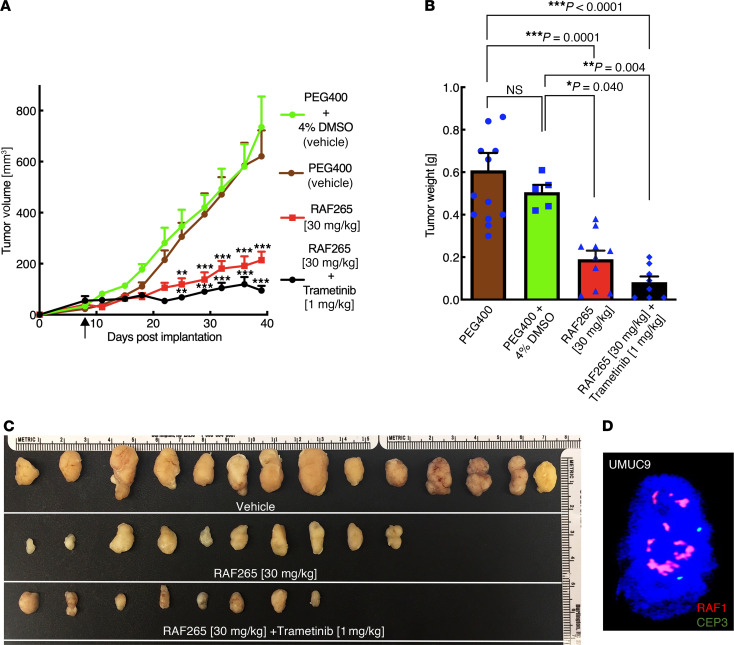
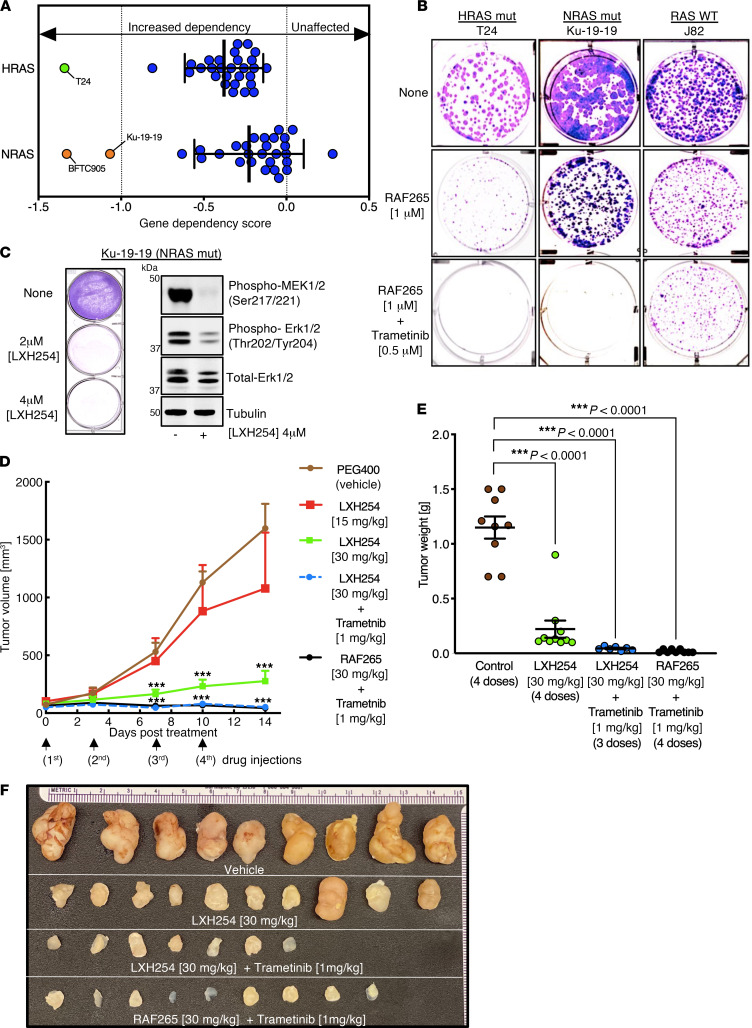
Bladder cancer is a genetically heterogeneous disease, and novel therapeutic strategies are needed to expand treatment options and improve clinical outcomes. Here, we identified a unique subset of urothelial tumors with focal amplification of the RAF1 (CRAF) kinase gene. RAF1-amplified tumors had activation of the RAF/MEK/ERK signaling pathway and exhibited a luminal gene expression pattern. Genetic studies demonstrated that RAF1-amplified tumors were dependent upon RAF1 activity for survival, and RAF1-activated cell lines and patient-derived models were sensitive to available and emerging RAF inhibitors as well as combined RAF plus MEK inhibition. Furthermore, we found that bladder tumors with HRAS- or NRAS-activating mutations were dependent on RAF1-mediated signaling and were sensitive to RAF1-targeted therapy. Together, these data identified RAF1 activation as a dependency in a subset making up nearly 20% of urothelial tumors and suggested that targeting RAF1-mediated signaling represents a rational therapeutic strategy.
Keywords: Cancer; Drug therapy; Oncogenes; Oncology.
Conflict of interest statement
Figures




Comment in
-
RAF1 amplification: an exemplar of MAPK pathway activation in urothelial carcinoma.J Clin Invest. 2021 Nov 15;131(22):e154095. doi: 10.1172/JCI154095. J Clin Invest. 2021. PMID: 34779406 Free PMC article.
-
Uro-Science.J Urol. 2022 Aug;208(2):468-469. doi: 10.1097/JU.0000000000002770. Epub 2022 May 20. J Urol. 2022. PMID: 35593059 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
