

Opioid-free anesthesia compared to opioid anesthesia for lung cancer patients undergoing video-assisted thoracoscopic surgery: A randomized controlled study
- PMID: 34555043
- PMCID: PMC8460000
- DOI: 10.1371/journal.pone.0257279
Opioid-free anesthesia compared to opioid anesthesia for lung cancer patients undergoing video-assisted thoracoscopic surgery: A randomized controlled study
Abstract
Background: Reducing intra-operative opioid consumption benefits patients by decreasing postoperative opioid-related adverse events. We assessed whether opioid-free anesthesia would provide effective analgesia-antinociception monitored by analgesia index in video-assisted thoracoscopic surgery.
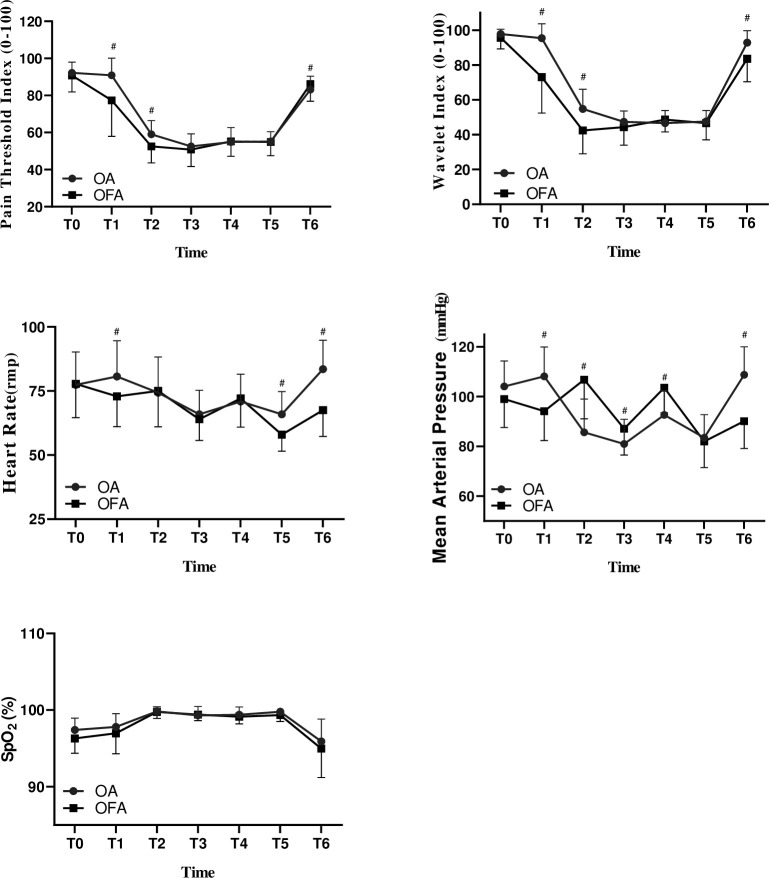
Methods: Patients (ASA Ⅰ-Ⅱ, 18-65 years old, BMI <30 kg m-2) scheduled to undergo video-assisted thoracoscopic surgery under general anesthesia were randomly allocated into two groups to receive opioid-free anesthesia (group OFA) with dexmedetomidine, sevoflurane plus thoracic paravertebral blockade or opioid-based anesthesia (group OA) with remifentanil, sevoflurane, and thoracic paravertebral blockade. The primary outcome variable was pain intensity during the operation, assessed by the depth of analgesia using the pain threshold index with the multifunction combination monitor HXD‑I. Secondary outcomes included depth of sedation monitoring by wavelet index and blood glucose concentration achieved from blood gas.
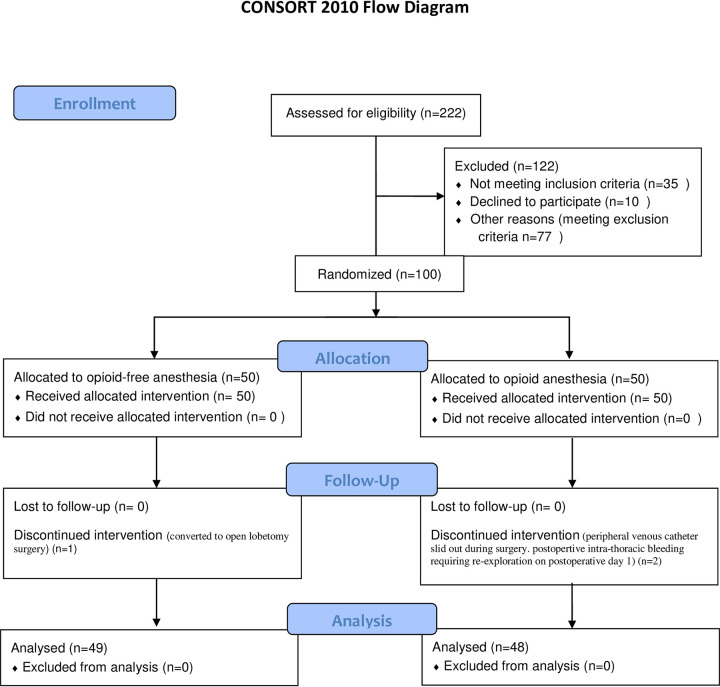
Results: One hundred patients were randomized; 3 patients were excluded due to discontinued intervention and 97 included in the final analysis. Intraoperative pain threshold index readings were not significantly different between group OFA and group OA from arriving operation room to extubation (P = 0.86), while the brain wavelet index readings in group OFA were notably lower than those in group OA from before general anesthesia induction to recovery of double lungs ventilation (P <0.001). After beginning of operation, the blood glucose levels in group OFA increased compared with baseline blood glucose values (P < 0.001). The recovery time and extubation time in group OFA were significantly longer than those in group OA (P <0.007).
Conclusions: This study suggested that our OFA regimen achieved equally effective intraoperative pain threshold index compared to OA in video-assisted thoracoscopic surgery. Depth of sedation was significantly deeper and blood glucose levels were higher with OFA. Study's limitations and strict inclusion criteria may limit the external validity of the study, suggesting the need of further randomized trials on the topic. Trial registration: ChiCTR1800019479, Title: "Opioid-free anesthesia in video-assisted thoracoscopic surgery lobectomy".
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Practice Guidelines for the Prevention, Detection, and Management of Respiratory Depression Associated with Neuraxial Opioid Administration: An Updated Report by the American Society of Anesthesiologists Task Force on Neuraxial Opioids and the American Society of Regional Anesthesia and Pain Medicine. Anesthesiology 2016;124:535–52. doi: 10.1097/ALN.0000000000000975 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
