

Whole genome sequencing in the diagnosis of primary ciliary dyskinesia
- PMID: 34556108
- PMCID: PMC8461892
- DOI: 10.1186/s12920-021-01084-w
Whole genome sequencing in the diagnosis of primary ciliary dyskinesia
Abstract
Background: It is estimated that 1-13% of cases of bronchiectasis in adults globally are attributable to primary ciliary dyskinesia (PCD) but many adult patients with bronchiectasis have not been investigated for PCD. PCD is a disorder caused by mutations in genes required for motile cilium structure or function, resulting in impaired mucociliary clearance. Symptoms appear in infancy but diagnosis is often late or missed, often due to the lack of a "gold standard" diagnostic tool and non-specific symptoms. Mutations in > 50 genes account for around 70% of cases, with additional genes, and non-coding, synonymous, missense changes or structural variants (SVs) in known genes presumed to account for the missing heritability.
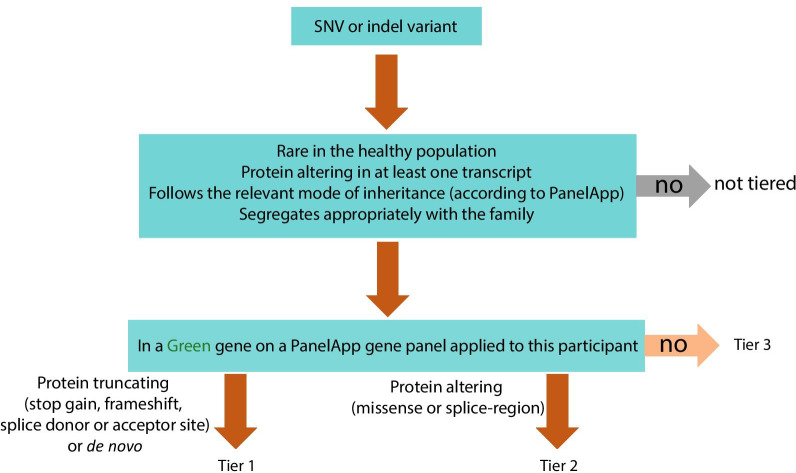
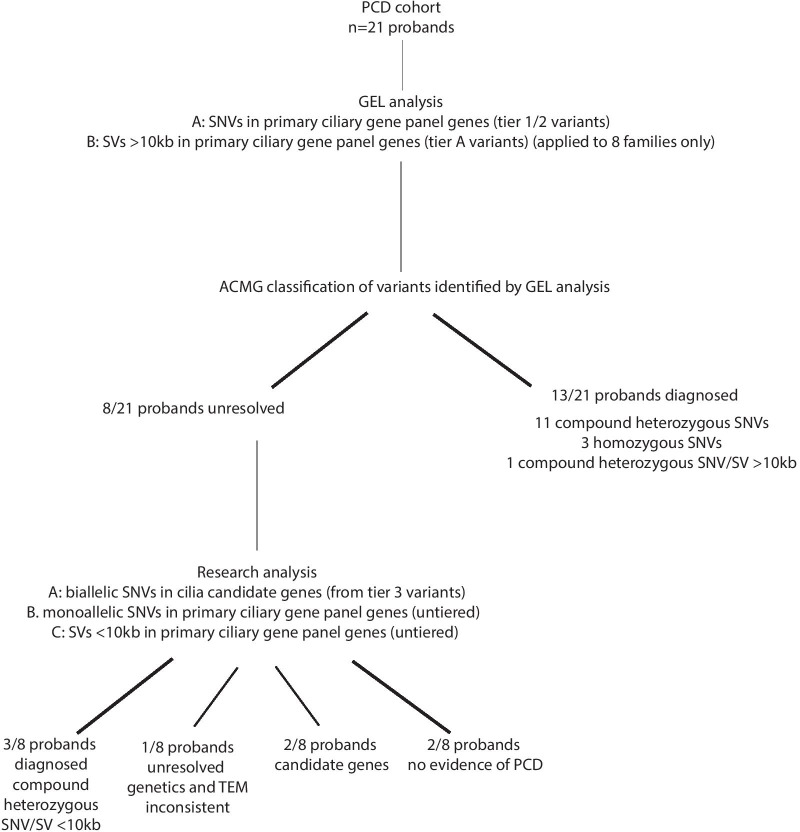
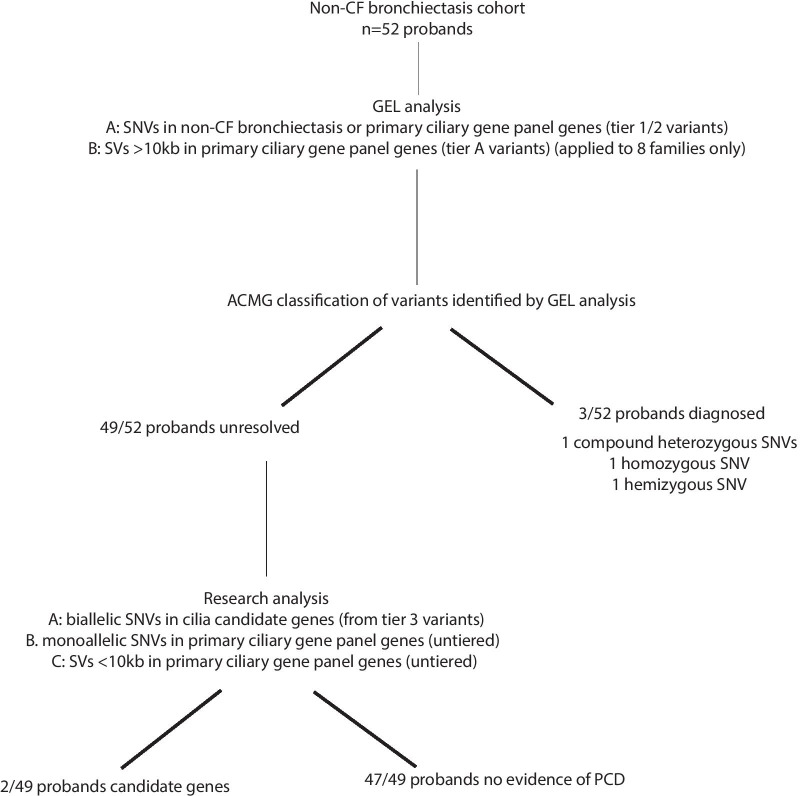
Methods: UK patients with no identified genetic confirmation for the cause of their PCD or bronchiectasis were eligible for whole genome sequencing (WGS) in the Genomics England Ltd 100,000 Genomes Project. 21 PCD probands and 52 non-cystic fibrosis (CF) bronchiectasis probands were recruited in Wessex Genome Medicine Centre (GMC). We carried out analysis of single nucleotide variants (SNVs) and SVs in all families recruited in Wessex GMC.
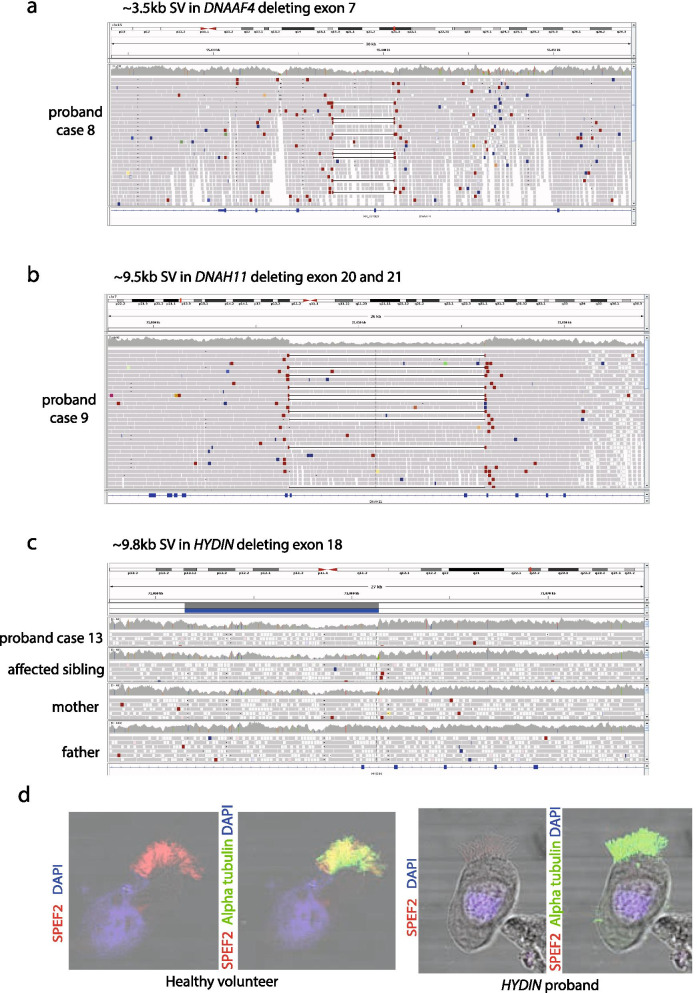
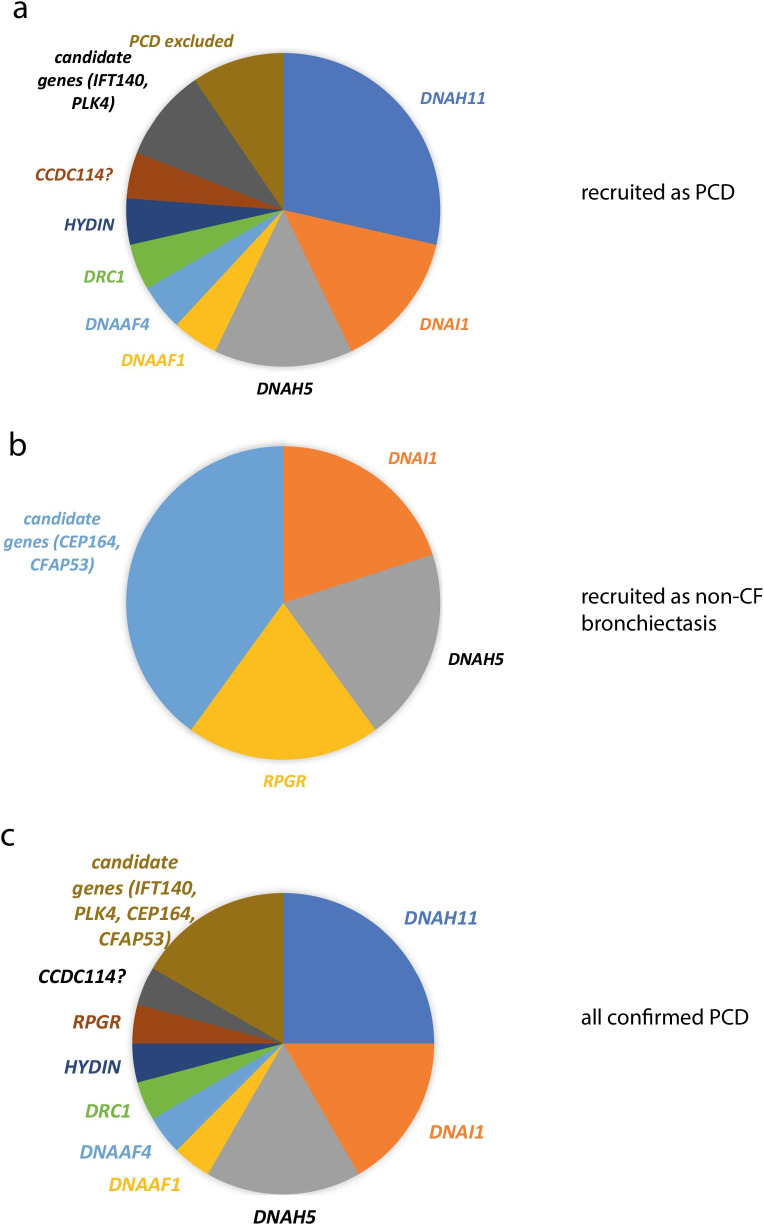
Results: 16/21 probands in the PCD cohort received confirmed (n = 9), probable (n = 4) or possible (n = 3) diagnosis from WGS, although 13/16 of these could have been picked up by current standard of care gene panel testing. In the other cases, SVs were identified which were missed by panel testing. We identified variants in novel PCD candidate genes (IFT140 and PLK4) in 2 probands in the PCD cohort. 3/52 probands in the non-CF bronchiectasis cohort received a confirmed (n = 2) or possible (n = 1) diagnosis of PCD. We identified variants in novel PCD candidate genes (CFAP53 and CEP164) in 2 further probands in the non-CF bronchiectasis cohort.
Conclusions: Genetic testing is an important component of diagnosing PCD, especially in cases of atypical disease history. WGS is effective in cases where prior gene panel testing has found no variants or only heterozygous variants. In these cases it may detect SVs and is a powerful tool for novel gene discovery.
Keywords: Diagnosis; Gene discovery; Non-CF bronchiectasis; Primary ciliary dyskinesia; Whole genome sequencing.
© 2021. The Author(s).
Conflict of interest statement
JSL reports grants, personal fees and non-financial support from Circassia. GW is employed by Illumina Inc. Other authors declare no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
