

Risk prediction of clinical adverse outcomes with machine learning in a cohort of critically ill patients with atrial fibrillation
- PMID: 34556682
- PMCID: PMC8460701
- DOI: 10.1038/s41598-021-97218-2
Risk prediction of clinical adverse outcomes with machine learning in a cohort of critically ill patients with atrial fibrillation
Abstract
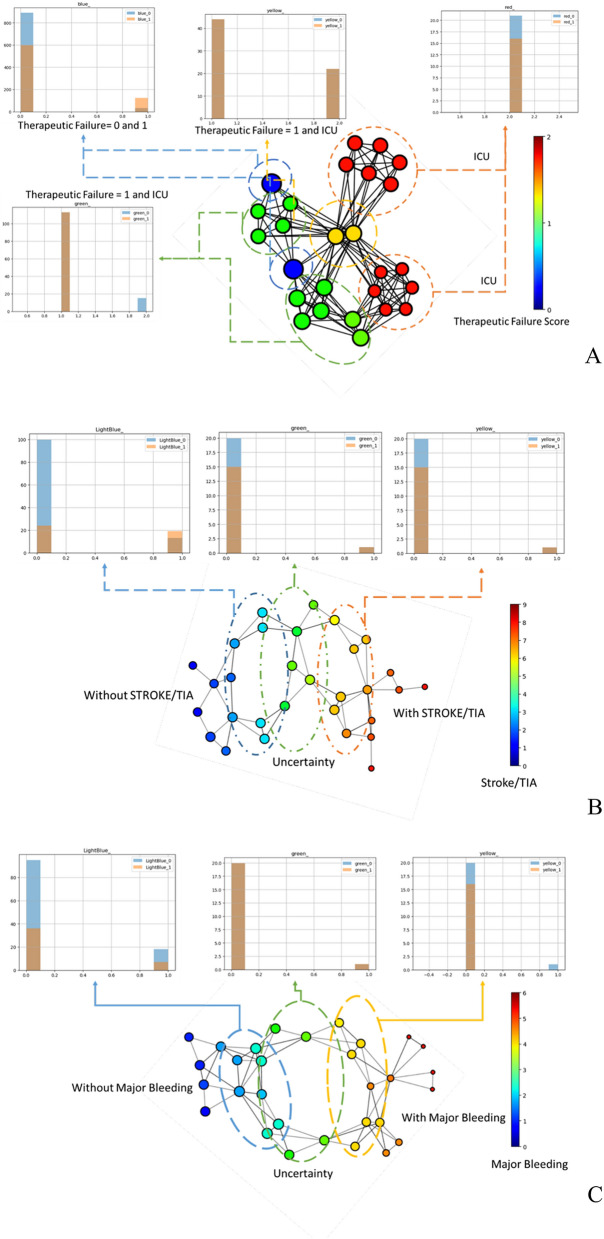
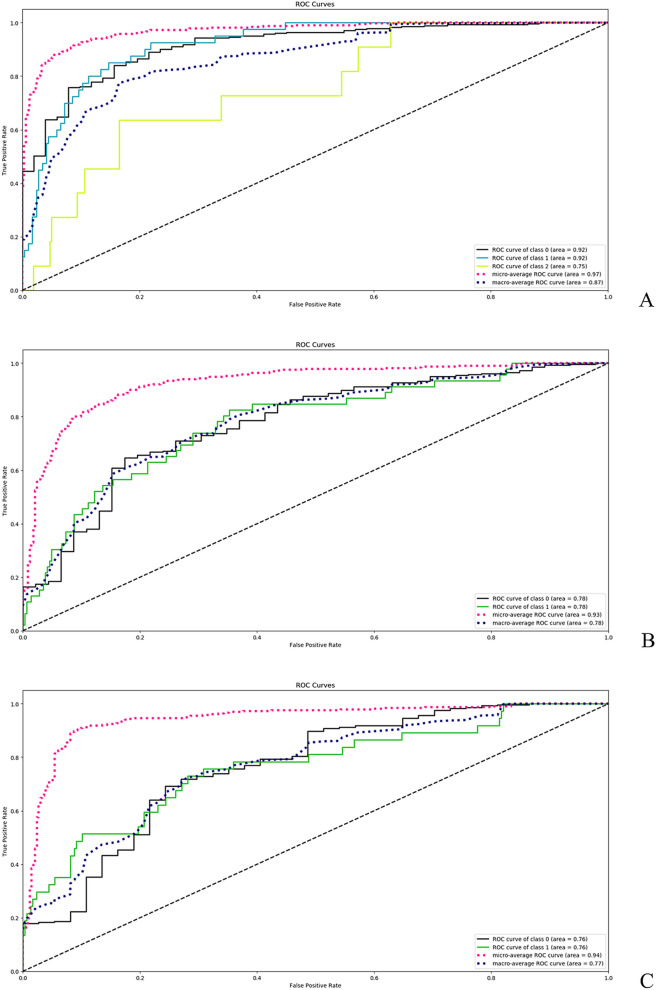
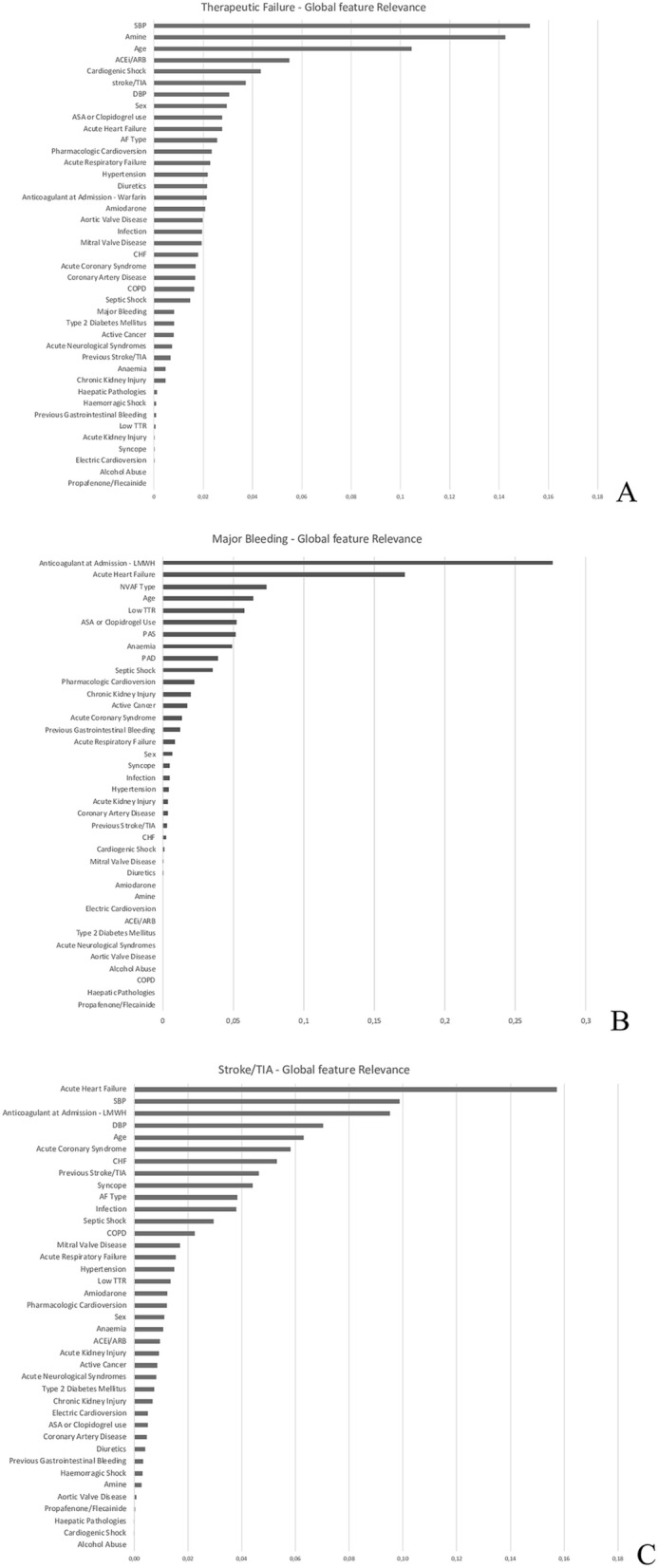
Critically ill patients affected by atrial fibrillation are at high risk of adverse events: however, the actual risk stratification models for haemorrhagic and thrombotic events are not validated in a critical care setting. With this paper we aimed to identify, adopting topological data analysis, the risk factors for therapeutic failure (in-hospital death or intensive care unit transfer), the in-hospital occurrence of stroke/TIA and major bleeding in a cohort of critically ill patients with pre-existing atrial fibrillation admitted to a stepdown unit; to engineer newer prediction models based on machine learning in the same cohort. We selected all medical patients admitted for critical illness and a history of pre-existing atrial fibrillation in the timeframe 01/01/2002-03/08/2007. All data regarding patients' medical history, comorbidities, drugs adopted, vital parameters and outcomes (therapeutic failure, stroke/TIA and major bleeding) were acquired from electronic medical records. Risk factors for each outcome were analyzed adopting topological data analysis. Machine learning was used to generate three different predictive models. We were able to identify specific risk factors and to engineer dedicated clinical prediction models for therapeutic failure (AUC: 0.974, 95%CI: 0.934-0.975), stroke/TIA (AUC: 0.931, 95%CI: 0.896-0.940; Brier score: 0.13) and major bleeding (AUC: 0.930:0.911-0.939; Brier score: 0.09) in critically-ill patients, which were able to predict accurately their respective clinical outcomes. Topological data analysis and machine learning techniques represent a concrete viewpoint for the physician to predict the risk at the patients' level, aiding the selection of the best therapeutic strategy in critically ill patients affected by pre-existing atrial fibrillation.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
