

Valsartan in early-stage hypertrophic cardiomyopathy: a randomized phase 2 trial
- PMID: 34556856
- PMCID: PMC8666141
- DOI: 10.1038/s41591-021-01505-4
Valsartan in early-stage hypertrophic cardiomyopathy: a randomized phase 2 trial
Abstract
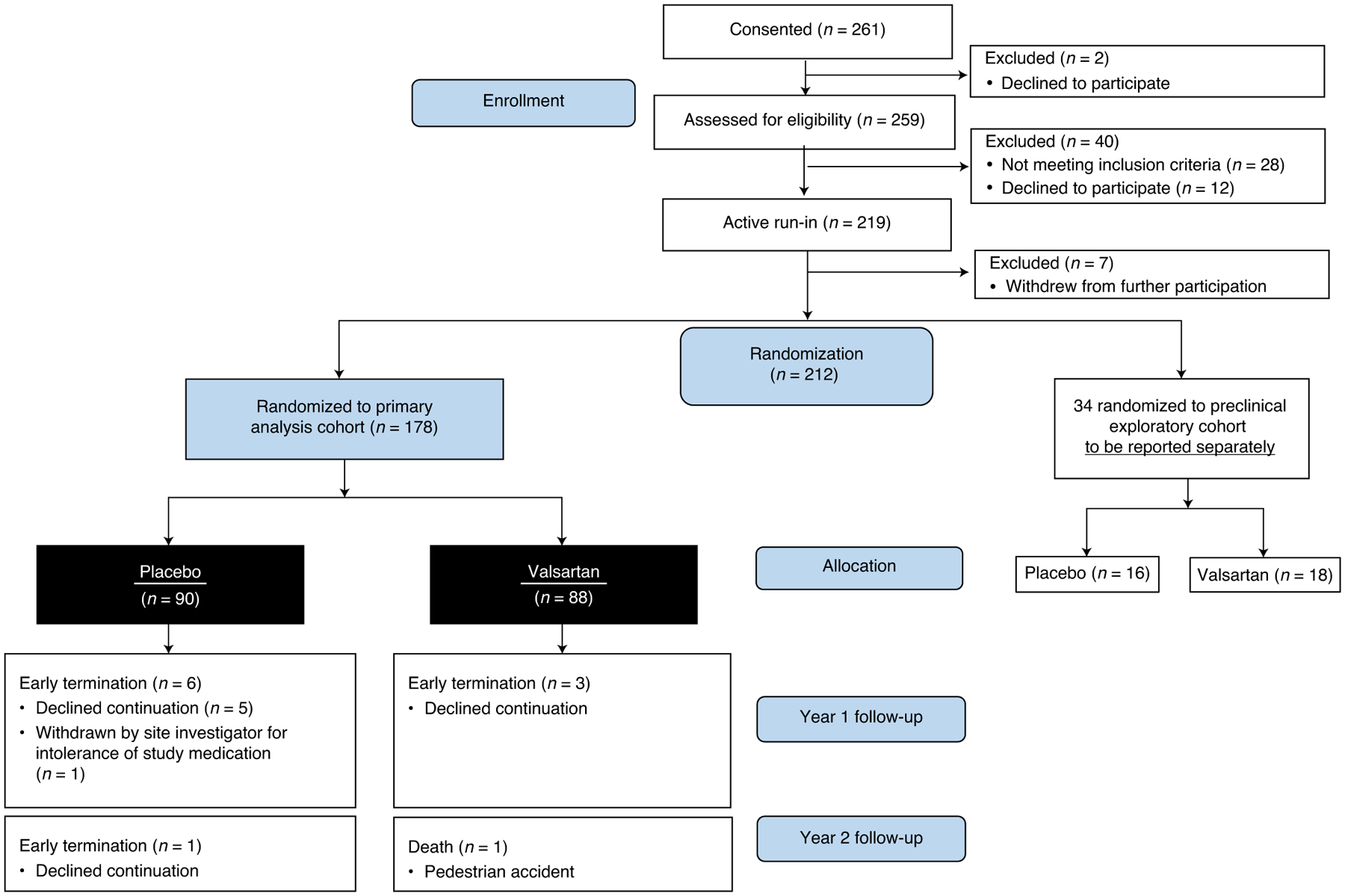
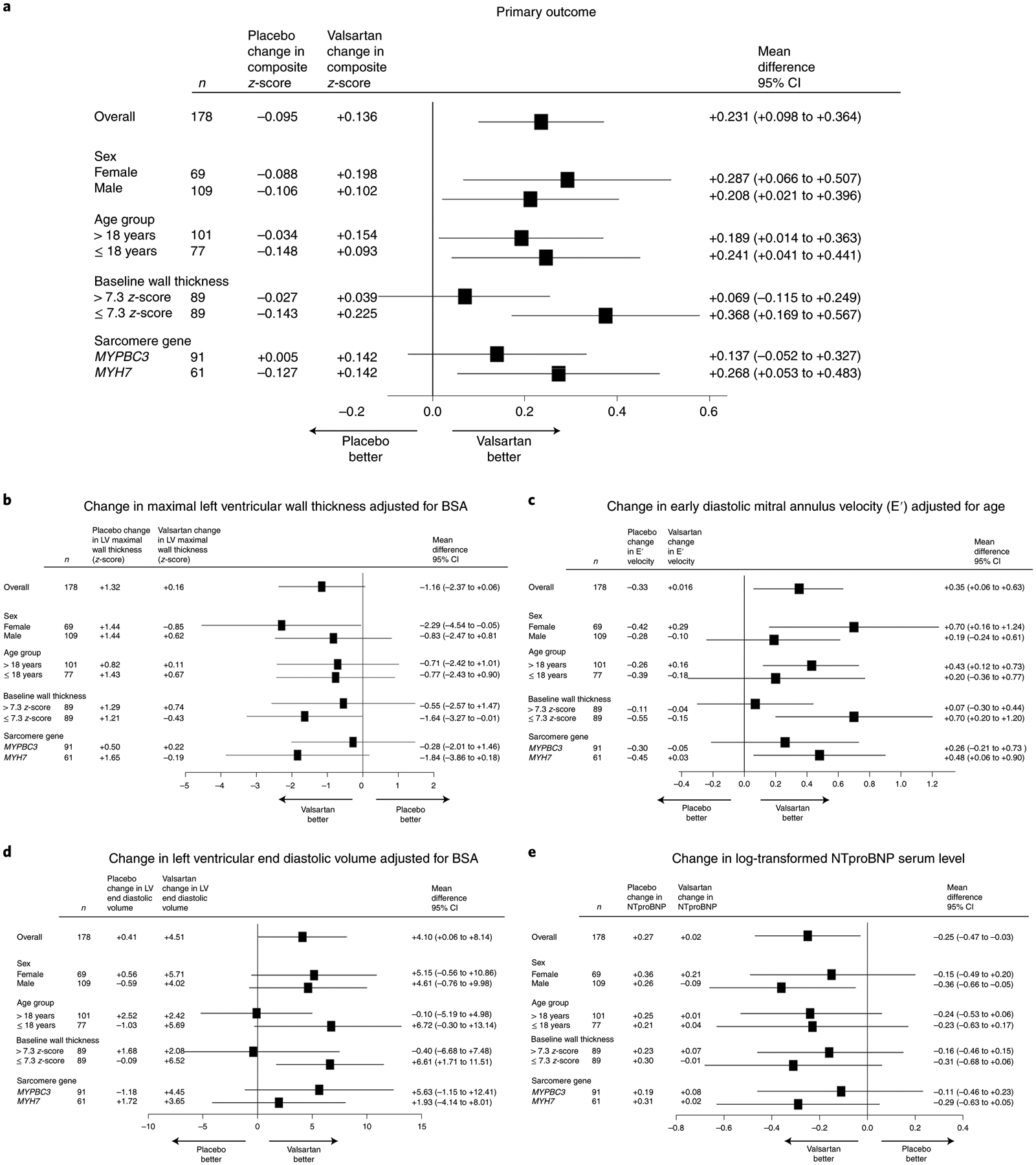
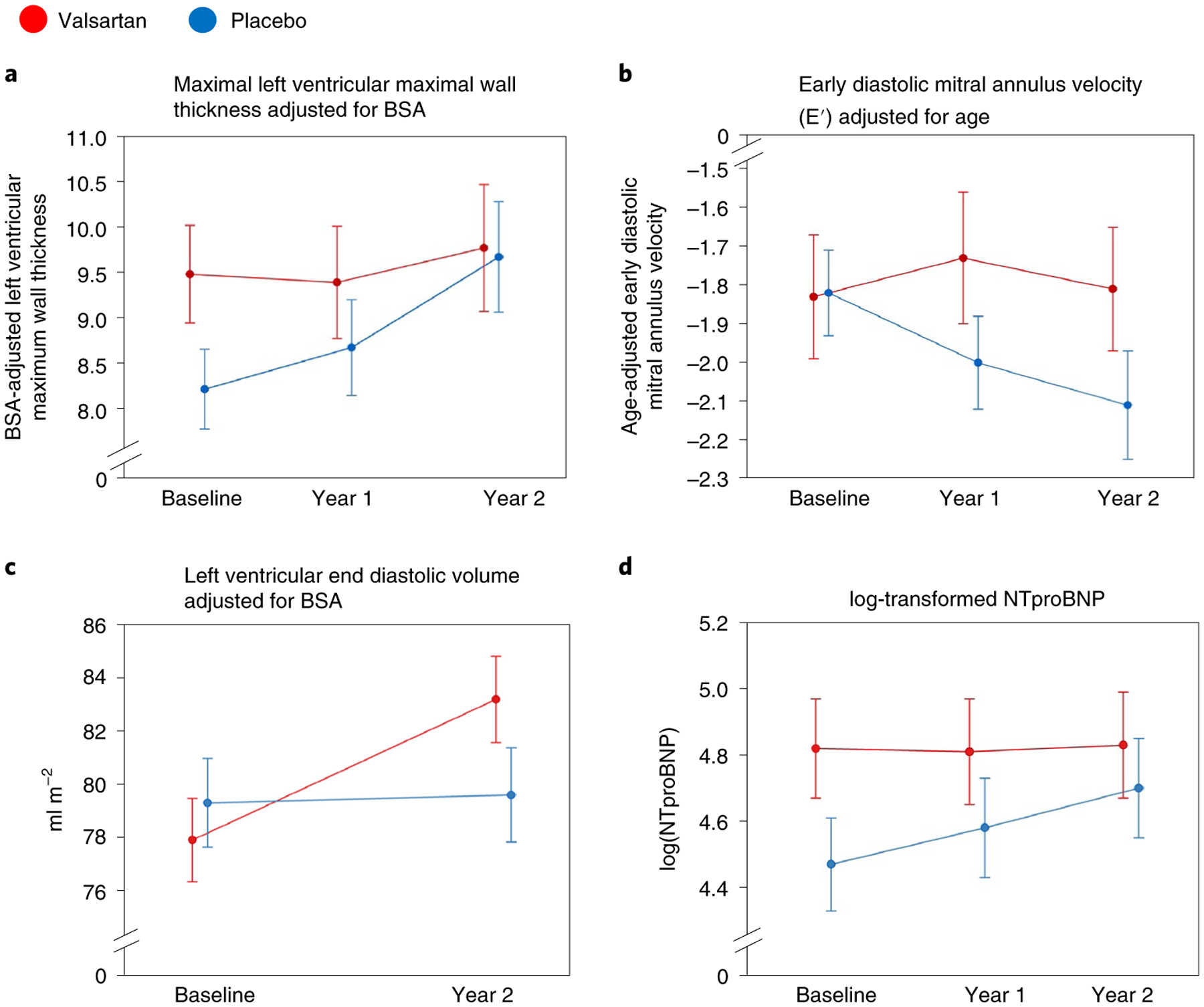
Hypertrophic cardiomyopathy (HCM) is often caused by pathogenic variants in sarcomeric genes and characterized by left ventricular (LV) hypertrophy, myocardial fibrosis and increased risk of heart failure and arrhythmias. There are no existing therapies to modify disease progression. In this study, we conducted a multi-center, double-blind, placebo-controlled phase 2 clinical trial to assess the safety and efficacy of the angiotensin II receptor blocker valsartan in attenuating disease evolution in early HCM. In total, 178 participants with early-stage sarcomeric HCM were randomized (1:1) to receive valsartan (320 mg daily in adults; 80-160 mg daily in children) or placebo for 2 years ( NCT01912534 ). Standardized changes from baseline to year 2 in LV wall thickness, mass and volumes; left atrial volume; tissue Doppler diastolic and systolic velocities; and serum levels of high-sensitivity troponin T and N-terminal pro-B-type natriuretic protein were integrated into a single composite z-score as the primary outcome. Valsartan (n = 88) improved cardiac structure and function compared to placebo (n = 90), as reflected by an increase in the composite z-score (between-group difference +0.231, 95% confidence interval (+0.098, +0.364); P = 0.001), which met the primary endpoint of the study. Treatment was well-tolerated. These results indicate a key opportunity to attenuate disease progression in early-stage sarcomeric HCM with an accessible and safe medication.
© 2021. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures
Comment in
-
Valsartan attenuates cardiac dysfunction and remodelling in patients with HCM.Nat Rev Cardiol. 2021 Dec;18(12):808. doi: 10.1038/s41569-021-00636-y. Nat Rev Cardiol. 2021. PMID: 34663946 No abstract available.
-
VANISHing the progression of cardiac abnormalities in hypertrophic cardiomyopathy with early use of valsartan?Eur Heart J. 2022 Jan 25;43(3):181-182. doi: 10.1093/eurheartj/ehab787. Eur Heart J. 2022. PMID: 35080239 No abstract available.
References
-
- Writing Committee M et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 142, e558–e631 (2020). - PubMed
-
- Kim JB et al. Polony multiplex analysis of gene expression (PMAGE) in mouse hypertrophic cardiomyopathy. Science 316, 1481–1484 (2007). - PubMed
-
- Lopez B, Gonzalez A & Diez J Circulating biomarkers of collagen metabolism in cardiac diseases. Circulation 121, 1645–1654 (2010). - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
