

Living Donor Versus Deceased Donor Pediatric Liver Transplantation: A Systematic Review and Meta-analysis
- PMID: 34557584
- PMCID: PMC8454909
- DOI: 10.1097/TXD.0000000000001219
Living Donor Versus Deceased Donor Pediatric Liver Transplantation: A Systematic Review and Meta-analysis
Abstract
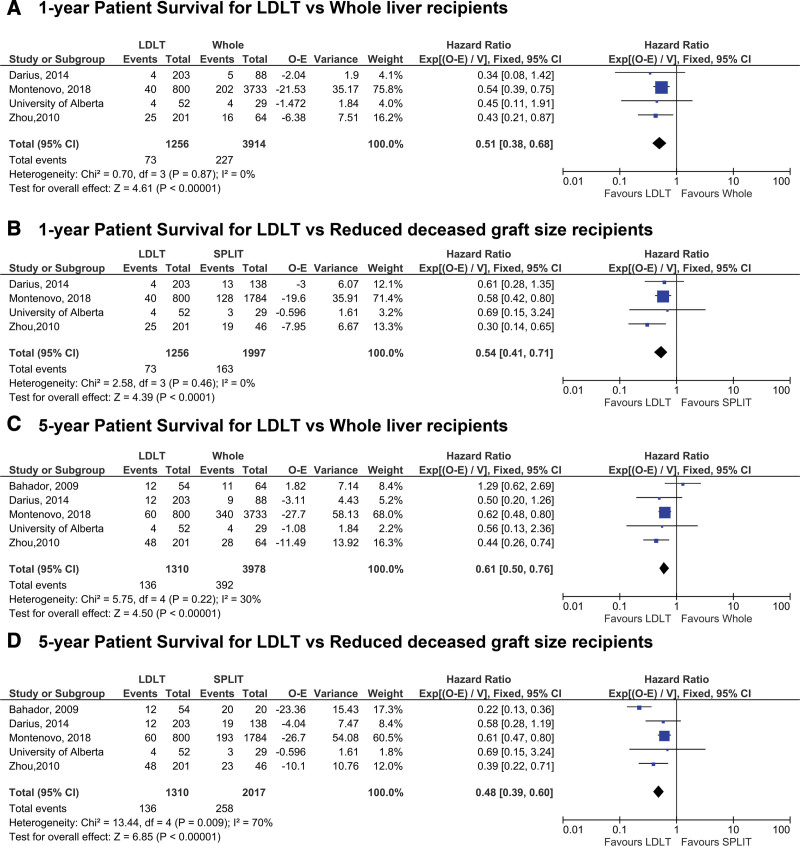
Reduced-size deceased donors and living donor liver transplantation (LDLT) can address the organ shortage for pediatric liver transplant candidates, but concerns regarding technical challenges and the risk of complications using these grafts have been raised. The aim of this study was to compare outcomes for pediatric LDLT and deceased donor liver transplantation (DDLT) via systematic review.
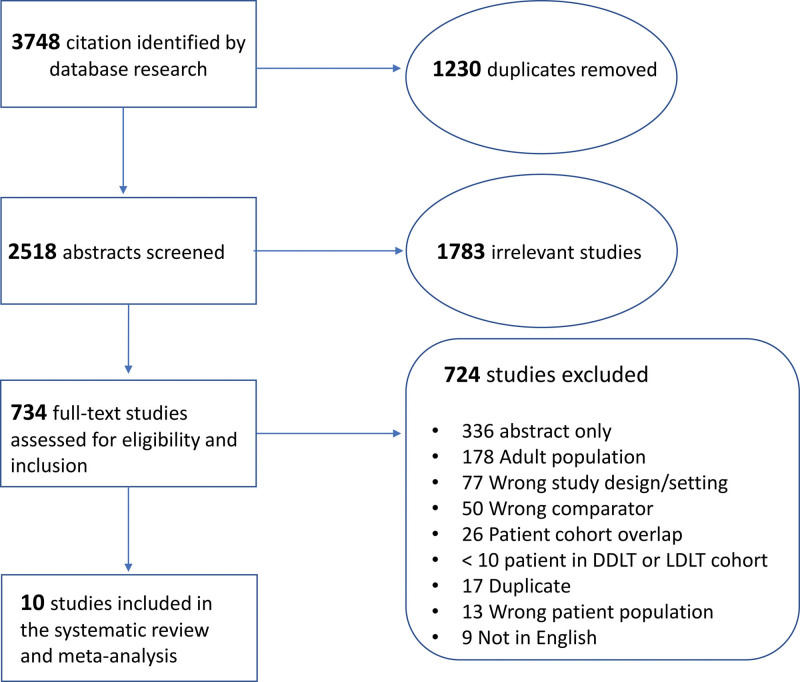
Methods: A systematic literature search was performed to identify studies reporting outcomes of pediatric (<18 y) LDLT and DDLT published between 2005 and 2019. A meta-analysis was conducted to examine peri- and postoperative outcomes using fixed- and random-effects models.
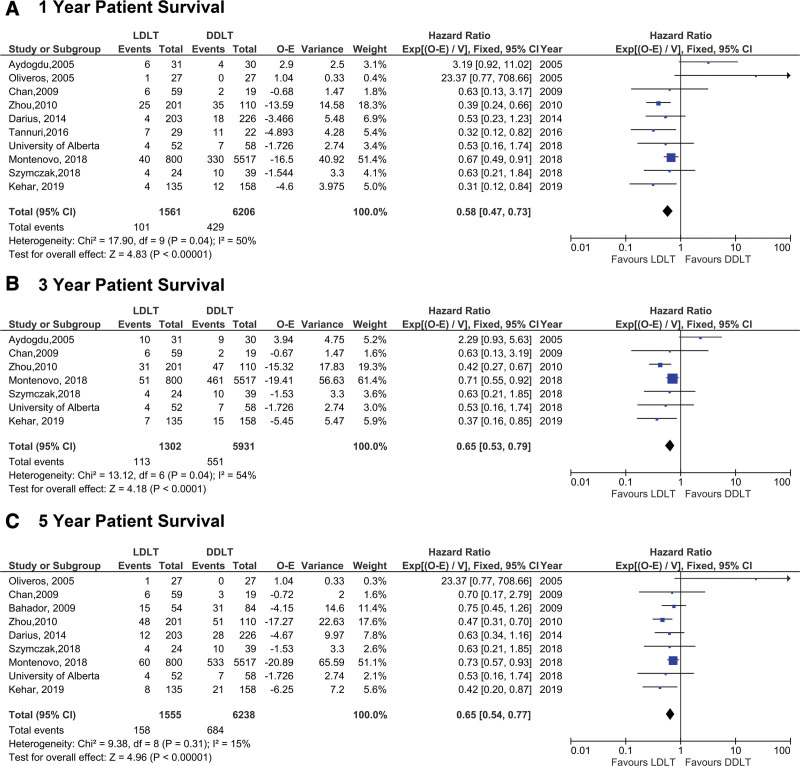
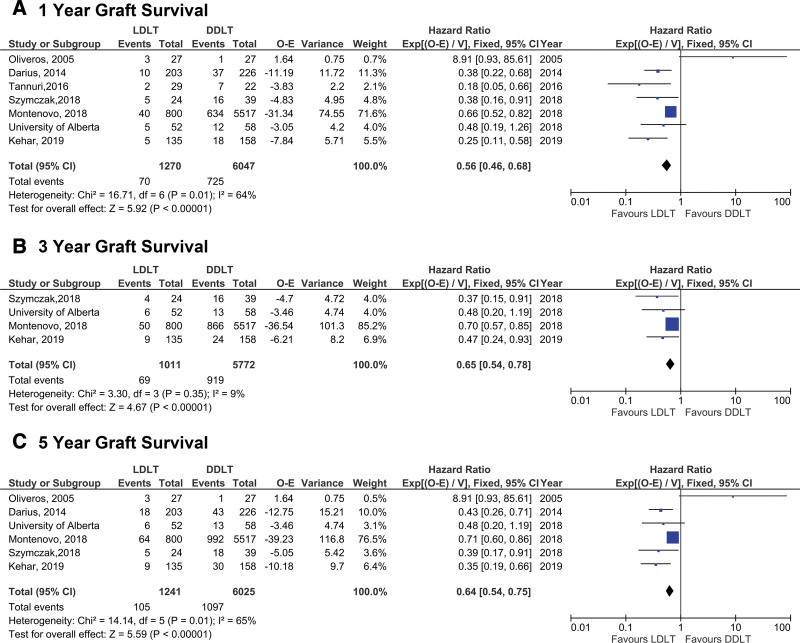
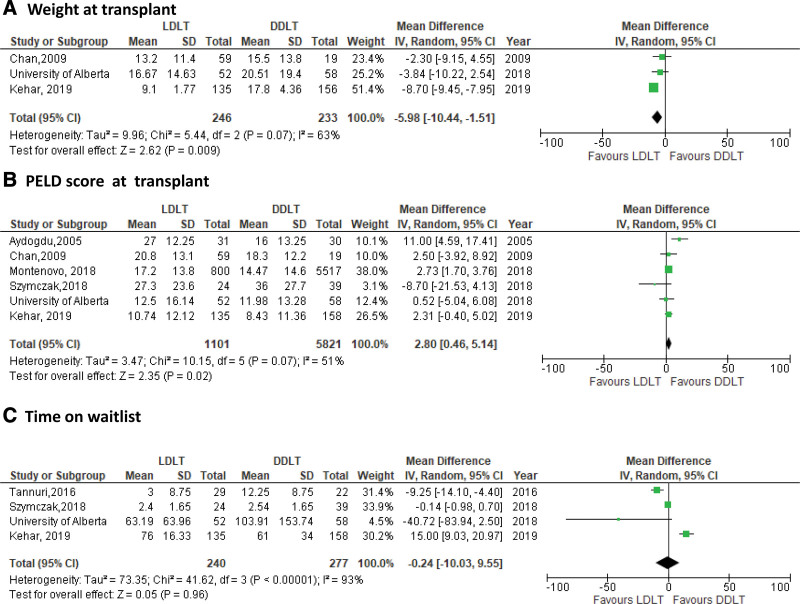
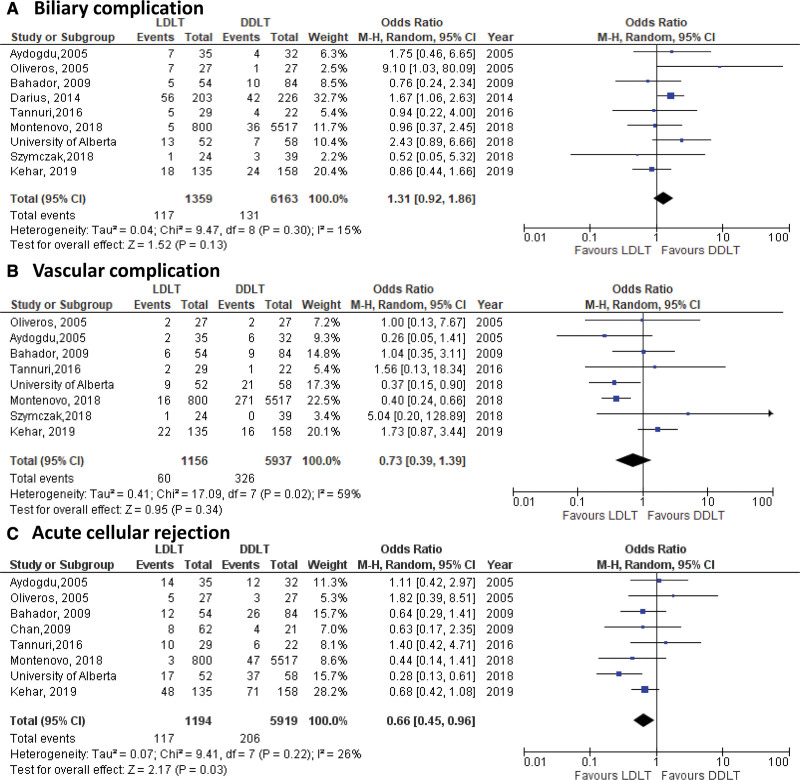
Results: Overall, 2518 abstracts were screened, and 10 studies met criteria for inclusion. In total, 1622 LDLT and 6326 DDLT pediatric patients from 4 continents were examined. LDLT resulted in superior patient survival when compared with DDLT at 1, 3, and 5 y post-LT (1-y hazard ratio: 0.58, 95% confidence interval [CI] 0.47-0.73, P < 0.0001). Similarly, LDLT resulted in superior graft survival at all time points post-LT when compared with DDLT (1-y hazard ratio: 0.56 [95% CI 0.46-0.68], P < 0.0001]. The OR for vascular complications was 0.73 (95% CI 0.39-1.39) and 1.31 (95% CI 0.92-1.86) for biliary complications in LDLT compared with DDLT, whereas LDLT was associated with lower rates of rejection (OR: 0.66 [95% CI 0.45-0.96], P = 0.03).
Conclusions: This meta-analysis demonstrates that LDLT may offer many advantages when compared with DDLT in children and suggests that LDLT should continue to be expanded to optimize outcomes for pediatric LT candidates.
Copyright © 2021 The Author(s). Transplantation Direct. Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no funding or conflicts of interest.
Figures
References
-
- Kwong A, Kim WR, Lake JR, et al. OPTN/SRTR 2018 annual data report: liver. Am J Transplant. 2020;20:193–299. - PubMed
-
- Cuenca AG, Kim HB, Vakili K. Pediatric liver transplantation. Semin Pediatr Surg. 2017;26:217–223. - PubMed
-
- Organ procurement and Transplantation Network. Build Advanced - OPTN. Available at https://optn.transplant.hrsa.gov/data/view-data-reports/build-advanced/. Accessed October 1, 2020.
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
