

Endovascular entry closure of a late type A aortic dissection after implantation of a self-expanding transcatheter heart valve (Evolut R): a case report
- PMID: 34557637
- PMCID: PMC8453414
- DOI: 10.1093/ehjcr/ytab343
Endovascular entry closure of a late type A aortic dissection after implantation of a self-expanding transcatheter heart valve (Evolut R): a case report
Abstract
Background: Late Stanford type A aortic dissections (TAADs) are a very rare complication after transcatheter aortic valve implantation (TAVI). Surgery is the treatment of choice, but perioperative mortality (25%) and neurological complications (18%) remain high.
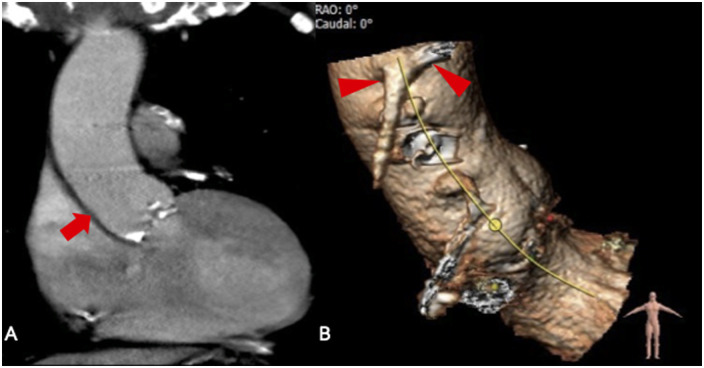
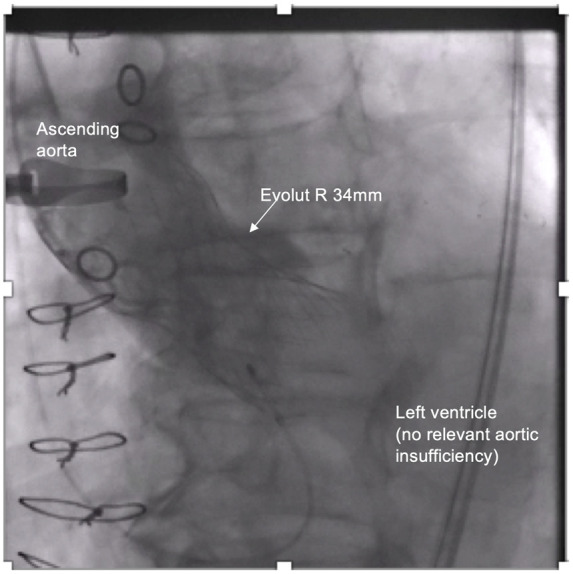
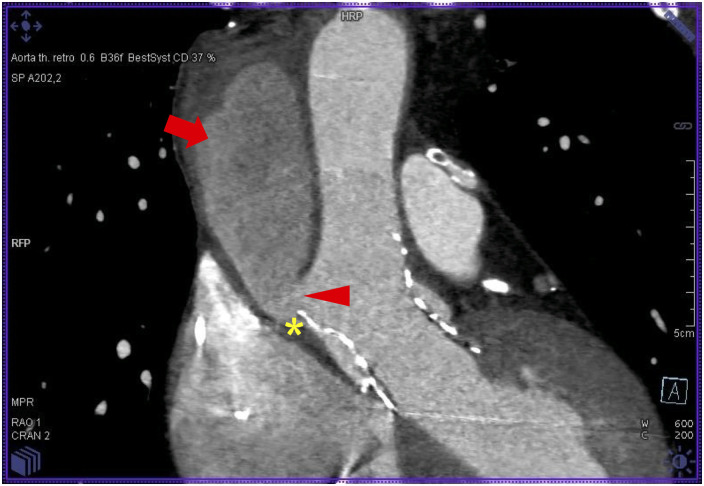
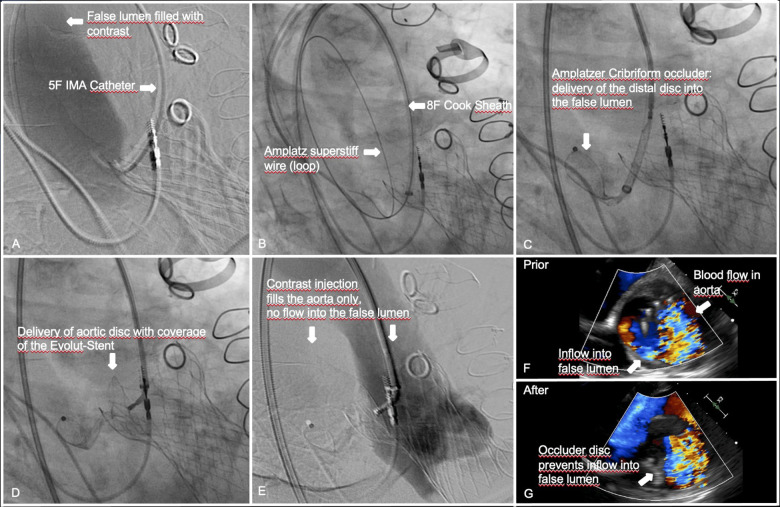
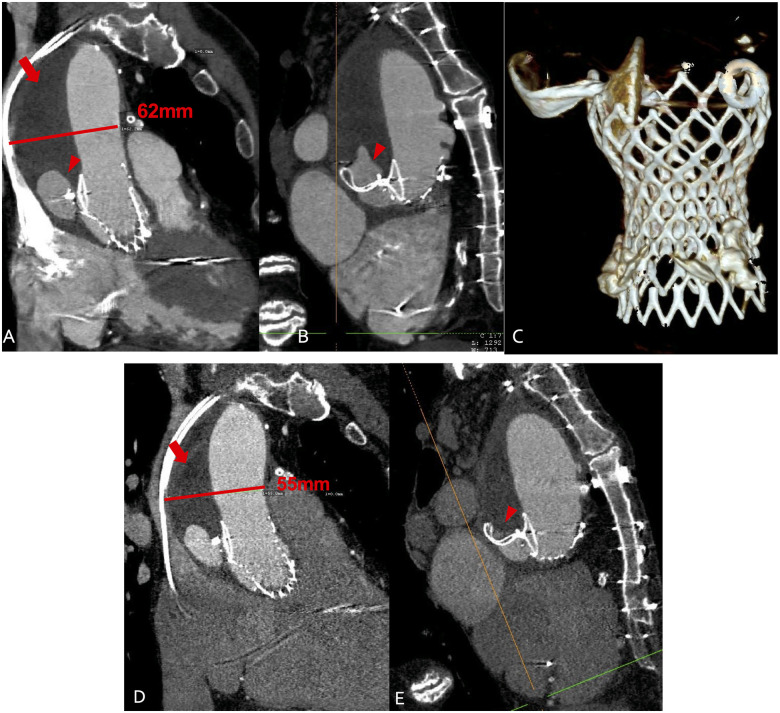
Case summary: An 85-year-old male patient presented with acute chest pain 5 months after a transfemoral Evolut R 34 mm transcatheter heart valve (THV) implantation. On multi-slice computed tomography (MSCT) a TAAD was found with a 7 mm primary entry at the supra-annular aortic edge of the THV expanding to the innominate artery without re-entry. Due to extensive comorbidities including two bypass operations in the history, the Heart Team declined surgery. Within 6 months of watchful waiting the maximal aortic diameter (MAD) increased from 57 to 62 mm. The decision was made to perform an endovascular closure of the inflow to the false lumen by implanting a 25 mm Amplatzer™ Cribriform Septal Occluder. MSCT 4 weeks after occlusion showed the false lumen almost completely filled with thrombus, MSCT 3 months later showed a MAD reduction to 55 mm with shrinkage of the false lumen.
Discussion: Presumably, the late TAAD was caused by the supra-annular edge of the Evolut-stent. Because of the extreme risk surgical repair was not an option and a stent graft would have occluded the vein grafts. This case shows that in absence of any other treatment options endovascular closure of the entry to the false lumen can be successfully performed in a TAAD after TAVI.
Keywords: Case report; Self-expanding transcatheter heart valve; Stanford type A aortic dissection; TAVI.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

References
-
- Bonser RS, Ranasinghe AM, Loubani M, Loubani M, Evans JD, Thalji NMA. et al. Evidence, lack of evidence, controversy, and debate in the provision and performance of the surgery of acute type A aortic dissection. J Am Coll Cardiol 2011;58:2455–2474. - PubMed
-
- Chiappini B, Schepens M, Tan E, Dell' Amore A, Morshuis W, Dossche K. et al. Early and late outcomes of acute type A aortic dissection: analysis of risk factors in 487 consecutive patients. Eur Heart J 2005;26:180–186. - PubMed
-
- Thomas M, Schymik G, Walther T, Himbert D, Lefèvre T, Treede H. et al. Thirty-day results of the SAPIEN aortic Bioprosthesis European Outcome (SOURCE) Registry: a European registry of transcatheter aortic valve implantation using the Edwards SAPIEN valve. Circulation 2010;122:62–69. - PubMed
-
- Langer NB, Hamid NB, Nazif TM, Khalique OK, Vahl TP, White J. et al. Injuries to the aorta, aortic annulus, and left ventricle during transcatheter aortic valve replacement. Circ Cardiovasc Interv 2017;10:e004735. - PubMed
-
- ESC Guidelines on the diagnosis and treatment of aortic diseases. Eur Heart J 2014;35:2873–2926. - PubMed
Publication types
LinkOut - more resources
Full Text Sources